
Research
Traditional Chinese Medicine—Review
Artemisinin,the Magic Drug Discovered from Traditional Chinese
Medicine
Jigang Wang a ,b ,c ,d ,#,Chengchao Xu c ,#,Yin Kwan Wong d ,#,Yujie Li a ,b ,Fulong Liao a ,b ,Tingliang Jiang a ,b ,Youyou Tu a ,b ,?
a
Artemisinin Research Center,China Academy of Chinese Medical Sciences,Beijing 100700,China
b
Institute of Chinese Materia Medica,China Academy of Chinese Medical Sciences,Beijing 100700,China c
Department of Pharmacology,Yong Loo Lin School of Medicine,National University of Singapore,Singapore 117600,Singapore d
Department of Physiology,Yong Loo Lin School of Medicine,National University of Singapore,Singapore 117597,Singapore
a r t i c l e i n f o Article history:
Received 8June 2018Revised 1August 2018
Accepted 12November 2018
Available online 18December 2018Keywords:Artemisinin
Mechanism of action Malaria Anti-cancer
a b s t r a c t
Artemisinin and its derivatives represent the most important and in?uential class of drugs in the ?ght against malaria. Since the discovery of artemisinin in the early 1970s, the global community has made great strides in characterizing and understanding this remarkable phytochemical and its unique chemical and pharmacological properties. Today, even as artemisinin continues to serve as the foundation for antimalarial therapy, numerous challenges have surfaced in the continued application and development of this family of drugs. These challenges include the emergence of delayed treatment responses to artemisinins in malaria and efforts to apply artemisinins for non-malarial indications. H ere, we provide an overview of the story of artemisinin in terms of its past, present, and future. In particular, we comment on the current understanding of the mechanism of action (MOA) of artemisinins, and emphasize the impor-tance of relating mechanistic studies to therapeutic outcomes, both in malarial and non-malarial contexts.
ó 2019 THE AUTHORS. Published by Elsevier LTD on behalf of Chinese Academy of Engineering and Higher Education Press Limited Company. This is an open access article under the CC BY-NC-ND license
1.Introduction
Malaria has been a debilitating disease with global in?uence since ancient times and continues to be one of the most wide-spread and damaging infectious diseases today [1].With the cause of disease having long been misattributed to ‘‘bad air,”the trans-missible and parasitic nature of malaria remained unknown until the works of Charles Louis Alphonse Laveran and Ronald Ross in the late 1800s.Their ?ndings established that protozoa belonging to the genus Plasmodium caused malaria,and that Anopheles mos-quitoes were the primary vectors of malarial infections.These observations made Laveran and Ross two of the earliest recipients of the Nobel Prize in Physiology or Medicine [2].
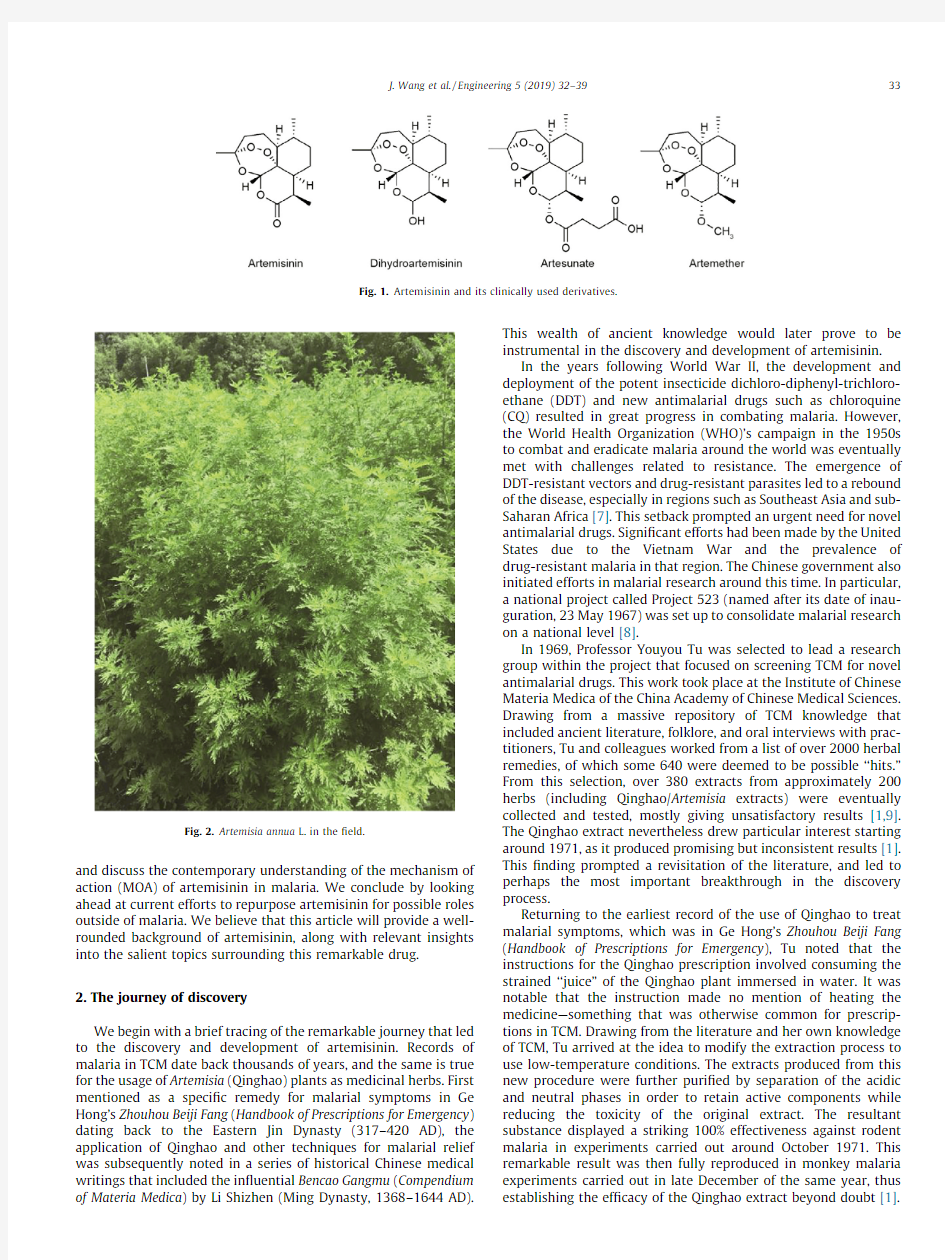
In the decades following their discoveries,ground-breaking progress has been made in the battle against the disease.The cru-sade launched by the Chinese government in the late 1960s to search for cures for malaria ultimately culminated in the discovery of artemisinin.Artemisinin (and its various derivatives,which we will refer to collectively as ‘‘artemisinin”unless otherwise speci-?ed)is a sesquiterpene lactone compound (Fig.1)with a unique chemical structure derived from the sweet wormwood plant,Artemisia annua L.(Fig.2).Since its discovery,it has become the most important and effective antimalarial drug [3].
In many ways,artemisinin is a truly fascinating drug.From the tumultuous process of its discovery,which was deeply tied to tra-ditional Chinese medicine (TCM),to its remarkable potency and impact as an antimalarial drug,it is not surprising that artemisinin has captured a great deal of attention since its introduction to the world stage [1].Over 40years after its discovery,artemisinin remains our bulwark against malaria and is the foundation of all major antimalarial therapies [4].Years of research spanning a range of disciplines have gone into the exploration and elucidation of the mechanisms of artemisinin in its antimalarial role [5].Beyond that,efforts have been made to repurpose artemisinin for non-malarial applications,thereby raising considerable anticipa-tion over the future development of this drug [6].
With that in mind,we feel that it is a good time to broadly review the timeline of this in?uential drug,spanning its past,present,and future.Beginning with a look back at the story of the discovery and development of artemisinin,we then review
?Corresponding author.
E-mail address:yytu@https://www.doczj.com/doc/8513572562.html, (Y.Tu).#
These authors contributed equally.
and discuss the contemporary understanding of the mechanism of action (MOA)of artemisinin in malaria.We conclude by looking ahead at current efforts to repurpose artemisinin for possible roles outside of malaria.We believe that this article will provide a well-rounded background of artemisinin,along with relevant insights into the salient topics surrounding this remarkable drug.2.The journey of discovery
We begin with a brief tracing of the remarkable journey that led to the discovery and development of artemisinin.Records of malaria in TCM date back thousands of years,and the same is true for the usage of Artemisia (Qinghao)plants as medicinal herbs.First mentioned as a speci?c remedy for malarial symptoms in Ge Hong’s Zhouhou Beiji Fang (Handbook of Prescriptions for Emergency )dating back to the Eastern Jin Dynasty (317–420AD),the application of Qinghao and other techniques for malarial relief was subsequently noted in a series of historical Chinese medical writings that included the in?uential Bencao Gangmu (Compendium of Materia Medica )by Li Shizhen (Ming Dynasty,1368–1644AD).
This wealth of ancient knowledge would later prove to be instrumental in the discovery and development of artemisinin.In the years following World War II,the development and deployment of the potent insecticide dichloro-diphenyl-trichloro-ethane (DDT)and new antimalarial drugs such as chloroquine (CQ)resulted in great progress in combating malaria.However,the World Health Organization (WHO)’s campaign in the 1950s to combat and eradicate malaria around the world was eventually met with challenges related to resistance.The emergence of DDT-resistant vectors and drug-resistant parasites led to a rebound of the disease,especially in regions such as Southeast Asia and sub-Saharan Africa [7].This setback prompted an urgent need for novel antimalarial drugs.Signi?cant efforts had been made by the United States due to the Vietnam War and the prevalence of drug-resistant malaria in that region.The Chinese government also initiated efforts in malarial research around this time.In particular,a national project called Project 523(named after its date of inau-guration,23May 1967)was set up to consolidate malarial research on a national level [8].
In 1969,Professor Youyou Tu was selected to lead a research group within the project that focused on screening TCM for novel antimalarial drugs.This work took place at the Institute of Chinese Materia Medica of the China Academy of Chinese Medical Sciences.Drawing from a massive repository of TCM knowledge that included ancient literature,folklore,and oral interviews with prac-titioners,Tu and colleagues worked from a list of over 2000herbal remedies,of which some 640were deemed to be possible ‘‘hits.”From this selection,over 380extracts from approximately 200herbs (including Qinghao/Artemisia extracts)were eventually collected and tested,mostly giving unsatisfactory results [1,9].The Qinghao extract nevertheless drew particular interest starting around 1971,as it produced promising but inconsistent results [1].This ?nding prompted a revisitation of the literature,and led to perhaps the most important breakthrough in the discovery process.
Returning to the earliest record of the use of Qinghao to treat malarial symptoms,which was in Ge Hong’s Zhouhou Beiji Fang (Handbook of Prescriptions for Emergency ),Tu noted that the instructions for the Qinghao prescription involved consuming the strained ‘‘juice”of the Qinghao plant immersed in water.It was notable that the instruction made no mention of heating the medicine—something that was otherwise common for prescrip-tions in TCM.Drawing from the literature and her own knowledge of TCM,Tu arrived at the idea to modify the extraction process to use low-temperature conditions.The extracts produced from this new procedure were further puri?ed by separation of the acidic and neutral phases in order to retain active components while reducing the toxicity of the original extract.The resultant substance displayed a striking 100%effectiveness against rodent malaria in experiments carried out around October 1971.This remarkable result was then fully reproduced in monkey malaria experiments carried out in late December of the same year,thus establishing the ef?cacy of the Qinghao extract beyond doubt [1]
.
Fig.1.Artemisinin and its clinically used
derivatives.
Fig.2.Artemisia annua L.in the ?eld.
J.Wang et al./Engineering 5(2019)32–3933
The breakthrough had been made,but the journey of drug development was by no means complete.Conditions in China at that time made it dif?cult to perform clinical trials of new drug candidates to ascertain their safety for humans.In an attempt to accelerate the process due to the seasonal and time-sensitive nat-ure of malarial research,Tu and colleagues decided to volunteer themselves as the?rst human subjects for toxicity and dose-?nding tests[8].This act established the safety pro?le of the Qinghao extract and enabled clinical trials to be carried out imme-diately,in the latter half of1972.The trials(which were carried out in Hainan Province and at the302Hospital PLA(now incorporated into the Fifth Medical Center of the Chinese PLA General Hospital) in Beijing)proved successful,and paved the way for Qinghao research to be pushed to the national level.A subsequent concerted effort on the part of the Chinese scienti?c community at large drove further research and development of Qinghao forward.The active component of the Qinghao extract,artemisinin(also known as Qinghaosu)itself,was isolated in November1972by Tu’s team at the Institute of Chinese Materia Medica.The team would later go on to develop dihydroartemisinin(DHA),which remains one of the most pharmacologically relevant derivatives today.In collabora-tion with other institutes across China,further groundwork in drug development,including the determination of the stereo-structure of artemisinin and further derivatization of artemisinin,was carried out in the following decade[10,11].These efforts,among others,culminated in the fourth meeting of the Scienti?c Working Group on the Chemotherapy of Malaria held in Beijing in1981, where the?ndings were presented by Tu for the?rst time.The results were published in1982as a series of papers under the name‘‘China Cooperative Research Group on Qinghaosu and Its Derivatives as Antimalarials”[12,13];thus the gift from Chinese medicine was delivered to the rest of the world.
In the subsequent years of the1980s,artemisinin and its deriva-tives were successfully employed in China to treat thousands of malaria patients[1].As the problem of drug-resistant malaria con-tinued to worsen elsewhere,it was not long before the commence-ment of clinical studies with artemisinin in other endemic regions in Asia[14–19].Consistent and encouraging results led to the expansion of such studies,particularly toward Africa[19–24]. The evidence was clear that artemisinin-based therapy,especially in combination with a slower-acting antimalarial such as me?o-quine or piperaquine,led to signi?cant improvements in parasite clearance and a rapid diminishing of symptoms for both uncompli-cated and severe Plasmodium falciparum malaria infection.At the same time,its tolerability was shown to be excellent,as reports of toxicity and safety concerns remained minimal[25].Across more than a decade’s worth of independent randomized clinical studies and meta-analyses,the outstanding ef?cacy and safety of artemisinin-based therapy became increasingly clear.Finally,in 2006,the WHO announced an alteration of its strategy to fully employ artemisinin combination therapies(ACTs)as the?rst-line treatment against malaria[26].ACTs remain the most effective and recommended antimalarial therapies today[4].
3.The search for a mechanism of action
It has been more than a decade since the implementation of ACTs as the of?cial?rst-line treatment for malaria and over three decades since the discovery of artemisinin.In this time,the clinical and pharmacological characteristics of artemisinin therapy have been extensively scrutinized and reported[27–30].Although the speci?cs of various derivatives can differ,artemisinin drugs are characterized by rapid action and potency,low toxicity,and a short half-life,which makes combination therapy with longer-acting antimalarial drugs ideal and recommended[30].Apart from its pharmacological properties,elucidating the MOA of a drug is important for optimizing treatment regimens.Dosages,drug com-binations,and even considerations of drug resistance are closely related to the molecular basis of a drug’s activity.It is thus some-what surprising that despite decades of widespread application, our understanding of the MOA of artemisinin remains fairly incom-plete.Here,we provide a brief overview of the prevailing under-standing as well as more recent developments in mechanistic studies of artemisinin[31,32].In general,the outstanding thera-peutic properties of artemisinin can be thought of as a result of two major processes:its unique mechanism of activation,and its downstream activity and drug targets.These mechanisms combine to yield a highly potent,yet highly speci?c,drug.
3.1.Drug activation
Artemisinin and its derivatives are sesquiterpene lactones that bear the1,2,4-trioxane moiety as the pharmacophore[33].In particular,the endoperoxide bridge within this group is well understood to be essential for the pharmacological activity of artemisinin[13,34,35].Artemisinins are prodrugs in two senses:?rst,many derivatives are rapidly converted to DHA in vivo,and second,their MOA depends on activation by cleavage of the endoperoxide bridge.The mechanism of this cleavage remains an issue in active research[36].Malarial parasites are characterized by extensive hemoglobin uptake and digestion during the erythrocytic stage of their life cycle[37,38].This releases copious amounts of free redox-active heme and free ferrous iron(Fe2+), which are thought to underlie the parasite speci?city of artemisi-nin.Indeed,hemoglobin digestion has been strongly linked with artemisinin susceptibility in parasites[38,39].Multiple models have been proposed with regard to the mechanism of endoperoxide cleavage by either free redox-active heme or free ferrous iron, and the downstream molecular events that follow cleavage [36,40–48].These proposals differ in terms of the nature of the cleavage and the identity of the reactive intermediates produced by drug activation.In general terms,however,they explain the parasite-speci?c drug activation through which reactive species are produced,leading to cellular damage and parasite killing. Recent evidence suggests that free redox-active heme may play a predominant role in drug activation[49,50].A2008study provided in vitro data that indicated that ferrous heme may be a stronger activator of artemisinin than other iron-containing species,includ-ing hemin,free ferrous iron,and undigested hemoglobin[49]. Similar observations were made in live parasites,in which artemisinin activation was blocked by inhibiting hemoglobin digestion but not by the chelation of free ferrous iron[47].Thus, the process of hemoglobin digestion in infected erythrocytes, which is required for parasite growth,is the key to the speci?city of artemisinin activation[38].
Interestingly,in studies using yeast cells as a proxy for malaria parasites[51,52],it was found that mitochondria were directly involved in both the activation and action of artemisinin,thus fur-ther linking artemisinin action to reactive oxidative species(ROS) production and oxidative damage.It is also plausible that multiple redundant activation pathways may exist in different environ-ments or localities,where the conditions and magnitude of activa-tion can differ[53].Looking ahead,it will be crucial to consider the pivotal role of drug activation in the activity of artemisinin and to further elucidate its mechanisms under different conditions.
3.2.Downstream mechanism
The crucial step in elucidating a drug’s MOA is to identify its cel-lular targets.In the conventional understanding of drug design and mechanisms,a drug modi?es one or more speci?c cellular targets, such as proteins,in order to effect downstream changes.However,
34J.Wang et al./Engineering5(2019)32–39
the exceedingly fast-acting and potent nature of artemisinin activ-ity,taken together with its ability to alkylate targets,may be due to quite a different mechanism.
First of all,heme releases from hemoglobin digestion functions that lie beyond drug activation,as previously outlined.Excess heme is converted in infected erythrocytes to hematin,which is toxic to the parasite via oxidative damage and direct lysis of cell membranes [54].Malarial parasites have therefore evolved a detoxifying mech-anism that converts hematin to the nontoxic and inert crystallized hemozoin via a biocrystallization process[55].Activated artemisi-nin has been reported to prevent the formation of hemozoin by alkylating heme;therefore,it functions in a similar capacity to other antimalarial drugs that act on hemozoin formation,such as CQ [45,56–58].Thus,free heme from hemoglobin digestion serves as both the activator and the target of artemisinin[45].
Given that activated artemisinin is thought to generate ROS,it is unsurprising that artemisinin has also been reported to directly alkylate protein targets[59,60].The translationally controlled tumor protein(TCTP)and the Plasmodium sarco/endoplasmic retic-ulum Ca2+-ATPase PfATP6were among the?rst targets of interest that were identi?ed as interacting partners of artemisinin [61–63].Consideration of the role of single targets in the activity of artemisinin has now evolved into MOAs that may depend on multiple targets,as later studies have shown[64–67].Using unbiased proteomics methods,it has been observed that artemisinin targeting may be promiscuous rather than monotarget-speci?c.In the?rst study that systematically reported artemisinin binding targets,over100proteins were identi?ed in live parasite strains [47].An independent study carried out by Ismail et al.[68]led to consistent?ndings.These results support a promiscuous mecha-nism of artemisinin targeting in which activated artemisinin alkylates and damages many cellular proteins,thereby disrupting multiple key biological functions and resulting in toxicity and lethality in parasites[47,48,50].Interestingly,PfATP6and other key transporters such as PfCRT and Pfmdr1are consistently labeled in these types of experiments.These?ndings are consistent with PfATP6being an important target for artemisinins[47,68].As an independent line of evidence,the mapped binding sites of artemi-sinin to TCTP further support a heme-activated promiscuous mechanism in which modi?cation sites are proximity-based and essentially random[50].
Our current knowledge of artemisinin paints a picture of a drug with a unique and elegant mechanism.Artemisinin and its deriva-tives are prodrugs that absolutely require endoperoxide group cleavage for drug activation and subsequent anti-parasite activity. Artemisinin activation is dependent on a heme-rich environment, which is speci?c to infected erythrocytes as well as being an unavoidable outcome of parasite metabolism.The heme-rich envi-ronment itself is then exploited by the activated drug to achieve ef?cient parasite killing.This mechanism essentially links infection and parasite growth to drug activation,thus ensuring both the out-standing speci?city and the tolerability of artemisinin therapy.At the same time,activated artemisinin indiscriminately damages proximal proteins and cellular structures.Rather than targeting a single protein or cellular function,like the majority of conventional drugs(including most antimalarials),artemisinin acts like a less-discriminative‘‘bomb”that detonates upon activation to cause widespread damage.The speci?city of artemisinin may therefore be seen to be based on its activation rather than on its targets. These unique properties of artemisinin make it almost the ideal weapon against malaria,especially in combination with other drugs that act via distinct mechanisms and complement the pharmacological pro?le of artemisinin.An obvious advantage of a promiscuously targeting drug is also worth noting here:The devel-opment of drug resistance is much more dif?cult when mutation in one or a few speci?c targets is not suf?cient to seriously impact drug activity.This advantage could well explain why artemisinin has remained generally ef?cacious despite its ubiquitous use over decades.
Nevertheless,recent trends have signaled the incidence and rise of malaria that is being cleared more slowly by ACTs,especially in the Asian endemic regions[69].This topic has been comprehen-sively covered from various angles by recent reviews and commen-taries[69–75].Regardless of the controversies about the exact de?nition of‘‘artemisinin resistance”in the?eld,the threat is undoubtedly real,given the place that artemisinin occupies in the control of malaria[76,77].To resolve this burning issue,two major challenges must be overcome:①A full understanding of the MOA of artemisinin must be achieved;and②the genetic and physiological features of the newly emerged artemisinin-resistant strains must be de?ned.Even though the MOA of artemisinin has been largely demysti?ed in the past few years, the molecular characterization of artemisinin-resistant malaria is far from clear.Continued efforts are required to achieve a complete picture of how artemisinin resistance relates to its mode of action. Based on this new knowledge,new therapeutic strategies can then be developed and tested.
4.Repurposing artemisinin
Artemisinin therapy is characterized by its outstanding tolera-bility and relative affordability.This combination of proven safety and accessibility make artemisinin a drug of exceptional interest for repurposing studies.Indeed,interest in non-malarial applications of artemisinin has increased steadily over time since artemisinin was?rst made known to the world[78].While malaria remains the only disease for which artemisinin is an approved treatment,the potential applications of artemisinin in anti-cancer,anti-in?ammatory,anti-parasitic(outside of malaria)and anti-viral roles,among others,have been explored in earnest over the years[78–82].Here,we brie?y comment on some promising research in artemisinin repurposing,especially in the?eld of cancer treatment,as a window into future drug development.
The ef?cacy of artemisinin in cancer cultures was?rst reported in1993,and has since been expanded on and extensively charac-terized[83–85].It is now well-reported that artemisinin and its derivatives display selective cytotoxicity against a range of cancer types in both in vitro and in vivo studies[86].Forays into clinical testing have been generally promising,if limited in number and scale[87–89].More than two decades of research on the basis of artemisinin action in cancer has uncovered a plethora of impli-cated targets and mechanisms.Artemisinin has been reported to induce mitochondrial apoptosis and other forms of cell death such as necroptosis,inhibit cancer angiogenesis and metastasis,and arrest the cancer cell cycle[90–97].These outcomes are reportedly mediated by a combination of oxidative damage,DNA damage, alteration of gene expression,and interactions with a wide array of signaling pathways including mammalian target of rapamycin (mTOR),NF-j B,mitogen-activated protein(MAP)kinases,and Wnt/b-catenin,among many others[82,98–102].These pathways and mechanisms have been extensively reviewed in recent publications[79–82].
While pathway validation is an important aspect of mechanistic study,it is also necessary to consider the big picture in terms of unifying drug activation and downstream activity in a manner similar to what was done in malaria studies.As is the case with malarial parasites,the activation mechanism of artemisinin in can-cer cells is likely to be heavily linked to its speci?city of action. Thus,the role of free ferrous iron versus free redox-active heme is once again being put under scrutiny,especially considering that iron is intimately linked to artemisinin-induced cytotoxicity in cancer[103,104].Recent studies have once again shed light on
J.Wang et al./Engineering5(2019)32–3935
the role of heme in artemisinin activation in cancer cells,thereby drawing parallels with the case in malaria.In particular,a range of methodologies have been used to demonstrate that modulation of heme synthesis and availability clearly correlates with cytotox-icity[105–108].It is also important to note that cancer cells have been reported to possess enhanced levels of heme metabolism and synthesis,and that this could underpin the cancer speci?city of artemisinin in a similar manner to the case in malaria[109–111].Speci?c targeting of artemisinin to mitochondria(the site of mammalian cell heme synthesis)or enhancement of heme levels by treatment with the heme precursor aminolevulinic acid(ALA) both improved anti-cancer activity[112–114].A heme-centric mechanism of activation and an iron-dependent mechanism of downstream cytotoxicity could possibly be a point of reconciliation between the roles of those two species in the anti-cancer activity of artemisinin[115].Further work to fully understand the basis of artemisinin speci?city in cancer will be critical for future therapeu-tic applications.
At the same time,it is necessary to consider the appropriate direction when moving forward in terms of validating artemisinin MOAs in cancer.Consider the case in malaria,where artemisinin is proposed to indiscriminately attack adjacent targets upon activa-tion.If artemisinin is activated in a similar manner in cancer cells, it is plausible that the same promiscuous multi-target mechanism would take place.This would explain the remarkable range of cel-lular effects and implicated pathways that have already been reported,as multiple targets and functional pathways are likely to be simultaneously affected by such a mechanism.Indeed,recent unbiased studies of artemisinin cancer targets using proteomics approaches have revealed a similar multi-target MOA by artemisi-nin in cancer cells[48,113,114].The mechanism of cytotoxicity itself is also a matter of great interest,especially with regard to non-apoptotic forms of cell death.Recent work has closely linked artemisinin-induced cytotoxicity to oxidative damage and lysoso-mal function,with a focus on the role of iron in contributing to the iron-dependent form of cell death known as ferroptosis [116–118].In particular,lysosome-mediated degradation of fer-ritin under autophagy conditions(termed ferritinophagy)releases free ferrous iron,which in turn contributes to both ferroptosis and iron-mediated generation of ROS[93,119].Autophagy itself is a cellular process that is reportedly activated by artemisinin,but has ambiguous effects on cancer cell survival and the cytotoxicity of artemisinin[115,119].It is clear that the relationship between autophagy,lysosomal activity,free ferrous iron,and iron-dependent ferroptotic cell death following artemisinin exposure represents a major area of uncertainty in the anti-cancer mecha-nism of artemisinin.However,efforts in unveiling novel,cancer-speci?c targets and mechanisms are steadily ongoing and continue to contribute to a grand view of artemisinin as an anti-cancer drug. Artemisinin-mediated effects on cancer stem cells,immunomodu-lation,cancer metastasis,cancer metabolism including the regula-tion of glycolysis,and a plethora of signaling pathways including signal transducer and activator of transcription3(STAT3),NF-j B, mTOR,and CREBP signaling are among recent reports,and indicate novel directions for further validation[115,120,121].In particular, the potential ability of artemisinin to serve as an immunomodula-tor in cancer by regulating regulatory T cell(Treg)activity and the production of pro-cancer-survival immunosuppressive cytokines such as prostaglandin E2(PGE2)is noteworthy,given the complex role of immunomodulatory drugs in cancer therapy[122–125]. Finally,efforts to improve the formulation and delivery of artemisinin-based drugs have shown promise in delivering enhanced ef?cacy and reduced susceptibility to drug resistance. These results include novel synthetic dimers,trimers,and drug conjugates(especially transferrin-conjugated systems),in addition to combination therapies;they represent an exciting ongoing area of research that has been reviewed comprehensively in recent publications[126–135].
In addition to the possible applications of artemisinin in cancer treatment,active research is taking place on its potential roles in addressing a range of other diseases.In particular,anti-in?ammatory effects against autoimmune diseases and allergic asthma,among other conditions,have been reported in a range of disease models[78].Some of these results correlate with observa-tions of immunosuppression in patients undergoing artemisinin therapy for malaria[136].Strong anti-viral effects of artemisinin have also been reported in herpes and in hepatitis B and C viruses, and other parasitic diseases including schistosomiasis have also been shown to respond to artemisinin treatment[137–141].Recent ?ndings have even identi?ed a remarkable—if controversial—role of artemisinin in diabetes through inducing transdifferentiation of pancreatic a cells to generate b cells[142,143].The MOA for these alternative applications is frequently discussed in terms of the canonical model of ROS generation and oxidative damage induction upon endoperoxide cleavage;however,non-canonical(including endoperoxide-independent)mechanisms have also been proposed, especially in the case of immunomodulation[78,144].It will be essential to pursue a clear view of how drug mechanisms and func-tions may differ under varying applications and conditions,while considering the importance of the conditions of drug activation.It is also worth noting that repurposing research might be best carried out in patients and regions that are not burdened with or at risk of malaria,in order to avoid possible interference or complications. Every care must be taken to ensure that the full potential of artemisinin can be realized without compromising its current applications.
5.Conclusion
The artemisinins are a class of remarkable drugs that have rede-?ned the landscape of antimalarial therapy.A combination of out-standing potency,safety,and accessibility has put artemisinin at the forefront of the ongoing battle against the malaria scourge, where it has already impacted millions of lives.Since its discovery, a concerted effort by the global community has assembled a pic-ture of a drug with a unique set of properties that makes it almost the ideal antimalarial drug.Active research in other?elds has also revealed a broad spectrum of promising applications for artemisi-nin outside of malaria.We believe that it is only logical to seek to maximize the utility of this drug in a range of capacities.In the context of malaria,doing so means to continue to clarify the mech-anisms of activation and action of artemisinin,while working to further improve its pharmacological properties both alone and in combination[145].Combined with a?rm grasp of the principles of artemisinin activity,this could be the key to clearing the uncer-tainties of artemisinin resistance.Such efforts would ensure that the drug can continue to perform in a similar or even greater capacity within the role that it has served for so long.Looking ahead,repurposing studies driven by a robust understanding of differential MOAs in different diseases and systems will also be instrumental in de?ning the future of artemisinin.Ultimately,it is our sincere hope that this gift from Chinese medicine can con-tinue to serve the pursuit of health for people all around the world, for many years to come.
Acknowledgements
This work was supported,in whole or in part,by the projects of the National Natural Science Foundation of China(81641002and 81473548);Major National Science and Technology Program of China for Innovative Drug(2017ZX09101002-001-001-05and
36J.Wang et al./Engineering5(2019)32–39
2017ZX09101002-001-001-3);and the Fundamental Research Funds for the Central Public Welfare Research Institutes (ZZ10-024and ZXKT18003).We would like to thank Dr.Lina Chen, Li Xiang,and Yuhua Shi for providing the photo of Artemisia annua L.We thank Prof.Sanjeev Krishna and Prof.Svetlana Tsogoeva for their valuable comments and assistance for polishing our manuscript.
Compliance with ethics guidelines
Jigang Wang,Chengchao Xu,Yin Kwan Wong,Yujie Li,Fulong Liao,Tingliang Jiang,and Youyou Tu declare that they have no con?ict of interest or?nancial con?icts to disclose.
References
[1]Tu Y.Artemisinin—a gift from traditional Chinese medicine to the world
(Nobel lecture).Angew Chem Int Ed2016;55(35):10210–26.
[2]Cox FE.History of the discovery of the malaria parasites and their vectors.
Parasit Vectors2010;3(1):5.
[3]Krishna S,Bustamante L,Haynes RK,Staines HM.Artemisinins:their growing
importance in medicine.Trends Pharmacol Sci2008;29(10):520–7.
[4]World Health Organization.World malaria report2017.Geneva:World
Health Organization;2017.
[5]Ding XC,Beck HP,Raso G.Plasmodium sensitivity to artemisinins:magic
bullets hit elusive targets.Trends Parasitol2011;27(2):73–81.
[6]Efferth T,Romero MR,Bilia AR,Osman AG,Sohly ME,et al.Expanding the
therapeutic spectrum of artemisinin:activity against infectious diseases beyond malaria and novel pharmaceutical developments.World J Tradit Chin Med2016;2(2):1–23.
[7]D’Alessandro U,Butti?ns H.History and importance of antimalarial drug
resistance.Trop Med Int Health2001;6(11):845–8.
[8]Tu Y.The discovery of artemisinin(Qinghaosu)and gifts from Chinese
medicine.Nat Med2011;17(10):1217–20.
[9]Liao F.Discovery of artemisinin(Qinghaosu).Molecules2009;14(12):5362–6.
[10]Collaboration Research Group for Qinghaosu.A new sesquiterpene lactone—
Qinghaosu.Chin Sci Bull1997;3:142.Chinese.
[11]Wang MY.Publication process involving the discovery of artemisinin
(Qinghaosu)https://www.doczj.com/doc/8513572562.html,n Pac J Trop Biomed2016;6(6):461–7.
[12]China Cooperative Research Group on Qinghaosu and Its Derivatives as
Antimalarials.Chemical studies on Qinghaosu(artemisinine).J Tradit Chin Med1982;2(1):3–8.Chinese.
[13]Klayman DL.Qinghaosu(artemisinin):an antimalarial drug from China.
Science1985;228(4703):1049–55.
[14]Jiang JB,Li GQ,Guo XB,Kong YC,Arnold K.Antimalarial activity of me?oquine
and https://www.doczj.com/doc/8513572562.html,ncet1982;2(8293):285–8.
[15]Looareesuwan S,Viravan C,Vanijanonta S,Wilairatana P,Suntharasamai P,
Charoenlarp P,et al.Randomised trial of artesunate and me?oquine alone and in sequence for acute uncomplicated falciparum https://www.doczj.com/doc/8513572562.html,ncet1992;339 (8797):821–4.
[16]Nosten F,Luxemburger C,ter Kuile FO,Woodrow C,Eh JP,
Chongsuphajaisiddhi T,et al.Treatment of multidrug-resistant Plasmodium falciparum malaria with3-day artesunate-me?oquine combination.J Infect Dis1994;170(4):971–7.
[17]Tran TH,Day NP,Nguyen HP,Nguyen TH,Tran TH,Pham PL,et al.A controlled
trial of artemether or quinine in Vietnamese adults with severe falciparum malaria.N Engl J Med1996;335(2):76–83.
[18]Looareesuwan S,Wilairatana P,Viravan C,Vanijanonta S,Pitisuttithum P,
Kyle DE.Open randomized trial of oral artemether alone and a sequential combination with me?oquine for acute uncomplicated falciparum malaria.
Am J Trop Med Hyg1997;56(6):613–7.
[19]Adjuik M,Babiker A,Garner P,Olliaro P,Taylor W,White N,et al;
International Artemisinin Study Group.Artesunate combinations for treatment of malaria:https://www.doczj.com/doc/8513572562.html,ncet2004;363(9402):9–17.
[20]Von Seidlein L,Jaffar S,Pinder M,Haywood M,Snounou G,Gemperli B,et al.
Treatment of African children with uncomplicated falciparum malaria with a new antimalarial drug,CGP56697.J Infect Dis1997;176(4):1113–6.
[21]Von Seidlein L,Bojang K,Jones P,Jaffar S,Pinder M,Obaro S,et al.A
randomized controlled trial of artemether/ben?umetol,a new antimalarial and pyrimethamine/sulfadoxine in the treatment of uncomplicated falciparum malaria in African children.Am J Trop Med Hyg1998;58
(5):638–44.
[22]Doherty JF,Sadiq AD,Bayo L,Alloueche A,Olliaro P,Milligan P,et al.A
randomized safety and tolerability trial of artesunate plus sulfadoxine—pyrimethamine versus sulfadoxine-pyrimethamine alone for the treatment of uncomplicated malaria in Gambian children.Trans R Soc Trop Med Hyg 1999;93(5):543–6.
[23]Dondorp AM,Fanello CI,Hendriksen IC,Gomes E,Seni A,Chhaganlal KD,et al;
AQUAMAT Group.Artesunate versus quinine in the treatment of severe falciparum malaria in African children(AQUAMAT):an open-label, randomised https://www.doczj.com/doc/8513572562.html,ncet2010;376(9753):1647–57.[24]WWARN Artemisinin based Combination Therapy(ACT)Africa Baseline
Study Group.Clinical determinants of early parasitological response to ACTs in African patients with uncomplicated falciparum malaria:a literature review and meta-analysis of individual patient data.BMC Med 2015;13:212.
[25]Efferth T,Kaina B.Toxicity of the antimalarial artemisinin and its derivatives.
Crit Rev Toxicol2010;40(5):405–21.
[26]World Health Organization.Guidelines for the treatment of
malaria.Geneva:World Health Organization;2006.
[27]Luo XD,Shen CC.The chemistry,pharmacology,and clinical applications of
Qinghaosu(artemisinin)and its derivatives.Med Res Rev1987;7(1):29–52.
[28]White NJ.Clinical pharmacokinetics and pharmacodynamics of artemisinin
and derivatives.Trans R Soc Trop Med Hyg1994;88(Suppl1):S41–3.
[29]De Vries PJ,Dien TK.Clinical pharmacology and therapeutic potential of
artemisinin and its derivatives in the treatment of malaria.Drugs1996;52
(6):818–36.
[30]German PI,Aweeka FT.Clinical pharmacology of artemisinin-based
combination therapies.Clin Pharmacokinet2008;47(2):91–102.
[31]Robert A,Dechy-Cabaret O,Cazelles J,Meunier B.From mechanistic studies
on artemisinin derivatives to new modular antimalarial drugs.Acc Chem Res 2002;35(3):167–74.
[32]Li J,Zhou B.Biological actions of artemisinin:insights from medicinal
chemistry studies.Molecules2010;15(8):1378–97.
[33]Van Agtmael MA,Eggelte TA,van Boxtel CJ.Artemisinin drugs in the
treatment of malaria:from medicinal herb to registered medication.Trends Pharmacol Sci1999;20(5):199–205.
[34]Meshnick SR,Taylor TE,Kamchonwongpaisan S.Artemisinin and the
antimalarial endoperoxides:from herbal remedy to targeted chemotherapy.
Microbiol Rev1996;60(2):301–15.
[35]Posner GH,O’Neill PM.Knowledge of the proposed chemical mechanism of
action and cytochrome p450metabolism of antimalarial trioxanes like artemisinin allows rational design of new antimalarial peroxides.Acc Chem Res2004;37(6):397–404.
[36]O’Neill PM,Barton VE,Ward SA.The molecular mechanism of action of
artemisinin—the debate continues.Molecules2010;15(3):1705–21.
[37]Lew VL,Tiffert T,Ginsburg H.Excess hemoglobin digestion and the osmotic
stability of Plasmodium falciparum-infected red blood cells.Blood2003;101
(10):4189–94.
[38]Klonis N,Crespo-Ortiz MP,Bottova I,Abu-Bakar N,Kenny S,Rosenthal PJ,
et al.Artemisinin activity against Plasmodium falciparum requires hemoglobin uptake and digestion.Proc Natl Acad Sci USA2011;108(28):11405–10. [39]Xie SC,Dogovski C,Hanssen E,Chiu F,Yang T,Crespo MP,et al.Haemoglobin
degradation underpins the sensitivity of early ring stage Plasmodium falciparum to artemisinins.J Cell Sci2016;129(2):406–16.
[40]Zhang F,Gosser DK Jr,Meshnick SR.Hemin-catalyzed decomposition of
artemisinin(Qinghaosu).Biochem Pharmacol1992;43(8):1805–9.
[41]Posner GH,Oh CH,Wang D,Gerena L,Milhous WK,Meshnick SR,et al.
Mechanism-based design,synthesis,and in vitro antimalarial testing of new 4-methylated trioxanes structurally related to artemisinin:the importance of
a carbon-centered radical for antimalarial activity.J Med Chem1994;37
(9):1256–8.
[42]Wu WM,Wu Y,Wu YL,Yao ZJ,Zhou CM,Li Y,et al.Uni?ed mechanistic
framework for the Fe(II)-induced cleavage of Qinghaosu and derivatives/ analogues.The?rst spin-trapping evidence for the previously postulated secondary C-4radical.J Am Chem Soc1998;120(14):3316–25.
[43]Stocks PA,Bray PG,Barton VE,Al-Helal M,Jones M,Araujo NC,et al.Evidence
for a common non-heme chelatable-iron-dependent activation mechanism for semisynthetic and synthetic endoperoxide antimalarial drugs.Angew Chem Int Ed2007;46(33):6278–83.
[44]Haynes RK,Chan WC,Lung CM,Uhlemann AC,Eckstein U,Taramelli D,et al.
The Fe2+-mediated decomposition,PfATP6binding,and antimalarial activities of artemisone and other artemisinins:the unlikelihood of C-centered radicals as bioactive intermediates.ChemMedChem2007;2(10):1480–97.
[45]Meunier B,Robert A.Heme as trigger and target for trioxane-containing
antimalarial drugs.Acc Chem Res2010;43(11):1444–51.
[46]Haynes RK,Cheu KW,N’Da D,Coghi P,Monti D.Considerations on the
mechanism of action of artemisinin antimalarials:part1—the‘carbon radical’and‘heme’hypotheses.Infect Disord Drug Targets2013;13(4):217–77. [47]Wang J,Zhang CJ,Chia WN,Loh CC,Li Z,Lee YM,et al.Haem-activated
promiscuous targeting of artemisinin in Plasmodium falciparum.Nat Commun 2015;6:10111.
[48]Zhou Y,Li W,Xiao Y.Pro?ling of multiple targets of artemisinin activated by
hemin in cancer cell proteome.ACS Chem Biol2016;11(4):882–8.
[49]Zhang S,Gerhard GS.Heme activates artemisinin more ef?ciently than
hemin,inorganic iron,or hemoglobin.Bioorg Med Chem2008;16
(16):7853–61.
[50]Li W,Zhou Y,Tang G,Xiao Y.Characterization of the artemisinin binding site
for translationally controlled tumor protein(TCTP)by bioorthogonal click chemistry.Bioconjug Chem2016;27(12):2828–33.
[51]Li W,Mo W,Shen D,Sun L,Wang J,Lu S,et al.Yeast model uncovers dual roles
of mitochondria in action of artemisinin.PLoS Genet2005;1(3):e36.
[52]Wang J,Huang L,Li J,Fan Q,Long Y,Li Y,et al.Artemisinin directly targets
malarial mitochondria through its speci?c mitochondrial activation.PLoS One 2010;5(3):e9582.
[53]Sun C,Li J,Cao Y,Long G,Zhou B.Two distinct and competitive pathways
confer the cellcidal actions of artemisinins.Microb Cell2015;2(1):14–25.
J.Wang et al./Engineering5(2019)32–3937
[54]Fitch CD,Chevli R,Kanjananggulpan P,Dutta P,Chevli K,Chou AC.Intracellular
ferriprotoporphyrin IX is a lytic agent.Blood1983;62(6):1165–8.
[55]Egan TJ.Recent advances in understanding the mechanism of hemozoin
(malaria pigment)formation.J Inorg Biochem2008;102(5–6):1288–99. [56]Cazelles J,Robert A,Meunier B.Alkylation of heme by artemisinin,an
antimalarial drug.Acad Sci Chem2001;4(2):85–9.
[57]Robert A,Benoit-Vical F,Claparols C,Meunier B.The antimalarial drug
artemisinin alkylates heme in infected mice.Proc Natl Acad Sci USA2005;102
(38):13676–80.
[58]Loup C,Lelièvre J,Benoit-Vical F,Meunier B.Trioxaquines and heme-
artemisinin adducts inhibit the in vitro formation of hemozoin better than chloroquine.Antimicrob Agents Chemother2007;51(10):3768–70.
[59]Yang YZ,Little B.Meshnick SR.Alkylation of proteins by artemisinin.Effects
of heme,pH,and drug structure.Biochem Pharmacol1994;48(3):569–73. [60]Meshnick SR.Artemisinin:mechanisms of action,resistance and toxicity.Int J
Parasitol2002;32(13):1655–60.
[61]Bhisutthibhan J,Pan XQ,Hossler PA,Walker DJ,Yowell CA,Carlton J,et al.The
Plasmodium falciparum translationally controlled tumor protein homolog and its reaction with the antimalarial drug artemisinin.J Biol Chem1998;273
(26):16192–8.
[62]Eckstein-Ludwig U,Webb RJ,Van Goethem ID,East JM,Lee AG,Kimura M,
et al.Artemisinins target the SERCA of Plasmodium falciparum.Nature 2003;424(9651):957–61.
[63]Uhlemann AC,Cameron A,Eckstein-Ludwig U,Fischbarg J,Iserovich P,Zuniga
FA,et al.A single amino acid residue can determine the sensitivity of SERCAs to artemisinins.Nat Struct Mol Biol2005;12(7):628–9.
[64]Krishna S,Pulcini S,Fatih F,Staines H.Artemisinins and the biological basis
for the PfATP6/SERCA hypothesis.Trends Parasitol2010;26(11):517–23. [65]Arnou B,Montigny C,Morth JP,Nissen P,Jaxel C,M?ller JV,et al.The
Plasmodium falciparum Ca2+-ATPase PfATP6:insensitive to artemisinin,but a potential drug target.Biochem Soc Trans2011;39(3):823–31.
[66]Cui L,Wang Z,Jiang H,Parker D,Wang H,Su XZ,et https://www.doczj.com/doc/8513572562.html,ck of association of
the S769N mutation in Plasmodium falciparum SERCA(PfATP6)with resistance to artemisinins.Antimicrob Agents Chemother2012;56
(5):2546–52.
[67]Krishna S,Pulcini S,Moore CM,Teo BH,Staines HM.Pumped up:re?ections on
PfATP6as the target for artemisinins.Trends Pharmacol Sci2014;35(1):4–11.
[68]Ismail HM,Barton V,Phanchana M,Charoensutthivarakul S,Wong MH,
Hemingway J,et al.Artemisinin activity-based probes identify multiple molecular targets within the asexual stage of the malaria parasites Plasmodium falciparum3D7.Proc Natl Acad Sci USA2016;113(8):2080–5. [69]Ashley EA,Dhorda M,Fairhurst RM,Amaratunga C,Lim P,Suon S,et al;
Tracking Resistance to Artemisinin Collaboration(TRAC).Spread of artemisinin resistance in Plasmodium falciparum malaria.N Eng J Med 2014;371(5):411–23.
[70]Dondorp AM,Yeung S,White L,Nguon C,Day NP,Socheat D,et al.Artemisinin
resistance:current status and scenarios for containment.Nat Rev Microbiol 2010;8(4):272–80.
[71]Paloque L,Ramadani AP,Mercereau-Puijalon O,Augereau JM,Benoit-Vical F.
Plasmodium falciparum:multifaceted resistance to artemisinins.Malar J 2016;15:149.
[72]Tilley L,Straimer J,Gn?dig NF,Ralph SA,Fidock DA.Artemisinin action and
resistance in Plasmodium falciparum.Trends Parasitol2016;32(9):682–96. [73]Wang J,Xu C,Lun ZR,Meshnick SR.Unpacking‘artemisinin resistance’.Trends
Pharmacol Sci2017;38(6):506–11.
[74]Gil JP,Krishna S.pfmdr1(Plasmodium falciparum multidrug drug resistance
gene1):a pivotal factor in malaria resistance to artemisinin combination therapies.Expert Rev Anti Infect Ther2017;15(6):527–43.
[75]Hanscheid T,Hardisty DW.How‘‘resistant”is artemisinin resistant
malaria?—The risks of ambiguity using the term‘‘resistant”malaria.Travel Med Infect Dis2018;24:23–4.
[76]Meshnick S.Perspective:artemisinin-resistant malaria and the wolf.Am J
Trop Med Hyg2012;87(5):783–4.
[77]World Health Organization.Artemisinin and artemisinin-based combination
therapy resistance.Report.Geneva:World Health Organization;2016Apr.
[78]Ho WE,Peh HY,Chan TK,Wong WS.Artemisinins:pharmacological actions
beyond anti-malarial.Pharmacol Ther2014;142(1):126–39.
[79]Firestone GL,Sundar SN.Anticancer activities of artemisinin and its bioactive
derivatives.Expert Rev Mol Med2009;11:e32.
[80]Crespo-Ortiz MP,Wei MQ.Antitumor activity of artemisinin and its
derivatives:from a well-known antimalarial agent to a potential anticancer drug.J Biomed Biotechnol2012;2012:247597.
[81]Lai HC,Singh NP,Sasaki T.Development of artemisinin compounds for cancer
treatment.Invest New Drugs2013;31(1):230–46.
[82]Efferth T.Artemisinin—second career as anticancer drug?World J Tradit Chin
Med2015;1(4):2–25.
[83]Woerdenbag HJ,Moskal TA,Pras N,MalingréTM,el-Feraly FS,Kampinga HH,
et al.Cytotoxicity of artemisinin-related endoperoxides to Ehrlich ascites tumor cells.J Nat Prod1993;56(6):849–56.
[84]Lai H,Singh NP.Selective cancer cell cytotoxicity from exposure to
dihydroartemisinin and holotransferrin.Cancer Lett1995;91(1):41–6. [85]Efferth T,Dunstan H,Sauerbrey A,Miyachi H,Chitambar CR.The anti-malarial
artesunate is also active against cancer.Int J Oncol2001;18(4):767–73. [86]Efferth T,Sauerbrey A,Olbrich A,Gebhart E,Rauch P,Weber HO,et al.
Molecular modes of action of artesunate in tumor cell lines.Mol Pharmacol 2003;64(2):382–94.
[87]Zhang ZY,Yu SQ,Miao LY,Huang XY,Zhang XP,Zhu YP,et al.Artesunate
combined with vinorelbine plus cisplatin in treatment of advanced non-small cell lung cancer:a randomized controlled trial.J Chin Integr Med2008;6
(2):134–8.
[88]Jansen FH,Adoubi I,JC KC,DE Cnodder T,Jansen N,Tschulakow A,et al.First
study of oral Artenimol-R in advanced cervical cancer:clinical bene?t, tolerability and tumor markers.Anticancer Res2011;31(12):4417–22. [89]Krishna S,Ganapathi S,Ster IC,Saeed ME,Cowan M,Finlayson C,et al.A
randomised,double blind,placebo-controlled pilot study of oral artesunate therapy for colorectal cancer.EBioMedicine2014;2(1):82–90.
[90]Efferth T,Rücker G,Falkenberg M,Manns D,Olbrich A,Fabry U,et al.
Detection of apoptosis in KG-1a leukemic cells treated with investigational drugs.Arzneimittelforschung1996;46(2):196–200.
[91]Willoughby JA Sr,Sundar SN,Cheung M,Tin AS,Modiano J,Firestone GL.
Artemisinin blocks prostate cancer growth and cell cycle progression by disrupting Sp1interactions with the cyclin-dependent kinase-4(CDK4) promoter and inhibiting CDK4gene expression.J Biol Chem2009;284
(4):2203–13.
[92]Steinbrück L,Pereira G,Efferth T.Effects of artesunate on cytokinesis and
G2/M cell cycle progression of tumour cells and budding yeast.Cancer Genomics Proteomics2010;7(6):337–46.
[93]Hamacher-Brady A,Stein HA,Turschner S,Toegel I,Mora R,Jennewein N,
et al.Artesunate activates mitochondrial apoptosis in breast cancer cells via iron-catalyzed lysosomal reactive oxygen species production.J Biol Chem 2011;286(8):6587–601.
[94]Anfosso L,Efferth T,Albini A,Pfeffer U.Microarray expression pro?les of
angiogenesis-related genes predict tumor cell response to artemisinins.
Pharmacogenomics J2006;6(4):269–78.
[95]Button RW,Lin F,Ercolano E,Vincent JH,Hu B,Hanemann CO,et al.
Artesunate induces necrotic cell death in schwannoma cells.Cell Death Dis 2014;5:e1466.
[96]Buommino E,Baroni A,Canozo N,Petrazzuolo M,Nicoletti R,Vozza A,et al.
Artemisinin reduces human melanoma cell migration by down-regulating
a V b3integrin and reducing metalloproteinase2production.Invest New
Drugs2009;27(5):412–8.
[97]Chen T,Li M,Zhang R,Wang H.Dihydroartemisinin induces apoptosis and
sensitizes human ovarian cancer cells to carboplatin therapy.J Cell Mol Med 2009;13(7):1358–70.
[98]Li PC,Lam E,Roos WP,Zdzienicka MZ,Kaina B,Efferth T.Artesunate derived
from traditional Chinese medicine induces DNA damage and repair.Cancer Res2008;68(11):4347–51.
[99]Hou J,Wang D,Zhang R,Wang H.Experimental therapy of hepatoma with
artemisinin and its derivatives:in vitro and in vivo activity,chemosensitization, and mechanisms of action.Clin Cancer Res2008;14(17):5519–30.
[100]Berdelle N,Nikolova T,Quiros S,Efferth T,Kaina B.Artesunate induces oxidative DNA damage,sustained DNA double-strand breaks,and the ATM/ ATR damage response in cancer cells.Mol Cancer Ther2011;10(12):2224–33. [101]Huang C,Ba Q,Yue Q,Li J,Li J,Chu R,et al.Artemisinin rewires the protein interaction network in cancer cells:network analysis,pathway identi?cation, and target prediction.Mol Biosyst2013;9(12):3091–100.
[102]Li X,Ba Q,Liu Y,Yue Q,Chen P,Li J,et al.Dihydroartemisinin selectively inhibits PDGFR a-positive ovarian cancer growth and metastasis through inducing degradation of PDGFR a protein.Cell Discov2017;3:17042. [103]Efferth T,Benakis A,Romero MR,Tomicic M,Rauh R,Steinbach D,et al.
Enhancement of cytotoxicity of artemisinins toward cancer cells by ferrous iron.Free Radic Biol Med2004;37(7):998–1009.
[104]Ba Q,Zhou N,Duan J,Chen T,Hao M,Yang X,et al.Dihydroartemisinin exerts its anticancer activity through depleting cellular iron via transferrin receptor-
1.PLoS One2012;7(8):e42703.
[105]Zhang S,Gerhard GS.Heme mediates cytotoxicity from artemisinin and serves as a general anti-proliferation target.PLoS One2009;4(10):e7472. [106]Stockwin LH,Han B,Yu SX,Hollingshead MG,ElSohly MA,Gul W,et al.
Artemisinin dimer anticancer activity correlates with heme-catalyzed reactive oxygen species generation and endoplasmic reticulum stress induction.Int J Cancer2009;125(6):1266–75.
[107]Zhang S,Chen H,Gerhard GS.Heme synthesis increases artemisinin-induced radical formation and cytotoxicity that can be suppressed by superoxide scavengers.Chem Biol Interact2010;186(1):30–5.
[108]Mercer AE,Copple IM,Maggs JL,O’Neill PM,Park BK.The role of heme and the mitochondrion in the chemical and molecular mechanisms of mammalian cell death induced by the artemisinin antimalarials.J Biol Chem2011;286
(2):987–96.
[109]Hooda J,Cadinu D,Alam MM,Shah A,Cao TM,Sullivan LA,et al.Enhanced heme function and mitochondrial respiration promote the progression of lung cancer cells.PLoS One2013;8(5):e63402.
[110]Hooda J,Shah A,Zhang L.Heme,an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes.Nutrients 2014;6(3):1080–102.
[111]Hooda J,Alam M,Zhang L.Measurement of heme synthesis levels in mammalian cells.J Vis Exp2015;101:e51579.
[112]Zhang X,Ba Q,Gu Z,Guo D,Zhou Y,Xu Y,et al.Fluorescent coumarin-artemisinin conjugates as mitochondria-targeting theranostic probes for enhanced anticancer activities.Chemistry2015;21(48):17415–21.
[113]Zhang CJ,Wang J,Zhang J,Lee YM,Feng G,Lim TK,et al.Mechanism-guided design and synthesis of a mitochondria-targeting artemisinin analogue with enhanced anticancer activity.Angew Chem Int Ed2016;55(44):13770–4.
38J.Wang et al./Engineering5(2019)32–39
[114]Wang J,Zhang J,Shi Y,Xu C,Zhang C,Wong YK,et al.Mechanistic investigation of the speci?c anticancer property of artemisinin and its combination with aminolevulinic acid for enhanced anticolorectal cancer activity.ACS Cent Sci2017;3(7):743–50.
[115]Wong YK,Xu C,Kalesh KA,He Y,Lin Q,Wong WSF,et al.Artemisinin as an anticancer drug:recent advances in target pro?ling and mechanisms of action.Med Res Rev2017;37(6):1492–517.
[116]Dixon SJ,Lemberg KM,Lamprecht MR,Skouta R,Zaitsev EM,Gleason CE,et al.
Ferroptosis:an iron-dependent form of nonapoptotic cell death.Cell 2012;149(5):1060–72.
[117]Eling N,Reuter L,Hazin J,Hamacher-Brady A,Brady NR.Identi?cation of artesunate as a speci?c activator of ferroptosis in pancreatic cancer cells.
Oncoscience2015;2(5):517–32.
[118]Ooko E,Saeed ME,Kadioglu O,Sarvi S,Colak M,Elmasaoudi K,et al.
Artemisinin derivatives induce iron-dependent cell death(ferroptosis)in tumor cells.Phytomedicine2015;22(11):1045–54.
[119]Yang ND,Tan SH,Ng S,Shi Y,Zhou J,Tan KS,et al.Artesunate induces cell death in human cancer cells via enhancing lysosomal function and lysosomal degradation of ferritin.J Biol Chem2014;289(48):33425–41.
[120]Efferth T.From ancient herb to modern drug:Artemisia annua and artemisinin for cancer therapy.Semin Cancer Biol2017;46:65–83.
[121]Abba ML,Patil N,Leupold JH,Saeed MEM,Efferth T,Allgayer H.Prevention of carcinogenesis and metastasis by artemisinin-type drugs.Cancer Lett 2018;429:11–8.
[122]Noori S,Hassan ZM.Dihydroartemisinin shift the immune response towards Th1,inhibit the tumor growth in vitro and in vivo.Cell Immunol2011;271
(1):67–72.
[123]Farsam V,Hassan ZM,Zavaran-Hosseini A,Noori S,Mahdavi M,Ranjbar M.
Antitumor and immunomodulatory properties of artemether and its ability to reduce CD4+CD25+FoxP3+T reg cells in vivo.Int Immunopharmacol 2011;11(11):1802–8.
[124]Zhang LX,Liu ZN,Ye J,Sha M,Qian H,Bu XH,et al.Artesunate exerts an anti-immunosuppressive effect on cervical cancer by inhibiting PGE2production and Foxp3expression.Cell Biol Int2014;38(5):639–46.
[125]Cui C,Feng H,Shi X,Wang Y,Feng Z,Liu J,et al.Artesunate down-regulates immunosuppression from colorectal cancer Colon26and RKO cells in vitro by decreasing transforming growth factor b1and interleukin-10.Int Immunopharmacol2015;27(1):110–21.
[126]Reiter C,Fr?hlich T,Gruber L,Hutterer C,Marschall M,Voigtl?nder C,et al.
Highly potent artemisinin-derived dimers and trimers:synthesis and evaluation of their antimalarial,antileukemia and antiviral activities.
Bioorg Med Chem2015;23(17):5452–8.
[127]Fr?hlich T,?apc?Karag?z A,Reiter C,Tsogoeva SB.Artemisinin-derived dimers:potent antimalarial and anticancer agents.J Med Chem2016;59
(16):7360–88.
[128]Fr?hlich T,Ndreshkjana B,Muenzner JK,Reiter C,Hofmeister E,Mederer S, et al.Synthesis of novel hybrids of thymoquinone and artemisinin with high activity and selectivity against colon cancer.ChemMedChem2017;12
(3):226–34.
[129]Efferth T.Cancer combination therapies with artemisinin-type drugs.
Biochem Pharmacol2017;139:56–70.[130]Fr?hlich T,Hahn F,Belmudes L,Leidenberger M,Friedrich O,Kappes B,et al.
Synthesis of artemisinin-derived dimers,trimers and dendrimers: investigation of their antimalarial and antiviral activities including putative mechanisms of action.Chemistry2018;24(32):8103–13.
[131]Horwedel C,Tsogoeva SB,Wei S,Efferth T.Cytotoxicity of artesunic acid homo-and heterodimer molecules toward sensitive and multidrug-resistant CCRF-CEM leukemia cells.J Med Chem2010;53(13):4842–8.
[132]Reiter C,Herrmann A,?apci A,Efferth T,Tsogoeva SB.New artesunic acid homodimers:potent reversal agents of multidrug resistance in leukemia cells.Bioorg Med Chem2012;20(18):5637–41.
[133]Reiter C,Capc?Karag?z A,Fr?hlich T,Klein V,Zeino M,Viertel K,et al.
Synthesis and study of cytotoxic activity of1,2,4-trioxane-and egonol-derived hybrid molecules against Plasmodium falciparum and multidrug-resistant human leukemia cells.Eur J Med Chem2014;75:403–12.
[134]Reiter C,Fr?hlich T,Zeino M,Marschall M,Bahsi H,Leidenberger M,et al.
New ef?cient artemisinin derived agents against human leukemia cells, human cytomegalovirus and Plasmodium falciparum:2nd generation1,2,4-trioxane-ferrocene hybrids.Eur J Med Chem2015;97:164–72.
[135]Leto I,Coronnello M,Righeschi C,Bergonzi MC,Mini E,Bilia AR.Enhanced ef?cacy of artemisinin loaded in transferrin-conjugated liposomes versus stealth liposomes against HCT-8colon cancer cells.ChemMedChem2016;11
(16):1745–51.
[136]Bunnag D,Viravan C,Looareesuwan S,Karbwang J,Harinasuta T.Clinical trial of artesunate and artemether on multidrug resistant falciparum malaria in Thailand.A preliminary report.Southeast Asian J Trop Med Public Health 1991;22(3):380–5.
[137]Efferth T,Romero MR,Wolf DG,Stamminger T,Marin JJ,Marschall M.The antiviral activities of artemisinin and artesunate.Clin Infect Dis2008;47
(6):804–11.
[138]Keiser J,Utzinger J.Artemisinins and synthetic trioxolanes in the treatment of helminth infections.Curr Opin Infect Dis2007;20(6):605–12.
[139]Saeed MEM,Krishna S,Greten HJ,Kremsner PG,Efferth T.Antischistosomal activity of artemisinin derivatives in vivo and in patients.Pharmacol Res 2016;110:216–26.
[140]Lam NS,Long X,Su XZ,Lu F.Artemisinin and its derivatives in treating helminthic infections beyond schistosomiasis.Pharmacol Res2018;133:77–100.
[141]Efferth T.Beyond malaria:the inhibition of viruses by artemisinin-type compounds.Biotechnol Adv2018;36(6):1730–7.
[142]Li J,Casteels T,Frogne T,Ingvorsen C,HonoréC,Courtney M,et al.
Artemisinins target GABAA receptor signaling and impair a cell identity.
Cell2017;168(1–2):86–100.e15.
[143]Van der Meulen T,Lee S,Noordeloos E,Donaldson CJ,Adams MW,Noguchi GM,et al.Artemether does not turn a cells into b cells.Cell Metab2018;27
(1).21825.e4.
[144]Ho WE,Cheng C,Peh HY,Xu F,Tannenbaum SR,Ong CN,et al.Anti-malarial drug artesunate ameliorates oxidative lung damage in experimental allergic asthma.Free Radic Biol Med2012;53(3):498–507.
[145]Isacchi B,Arrigucci S,la Marca G,Bergonzi MC,Vannucchi MG,Novelli A,et al.
Conventional and long-circulating liposomes of artemisinin:preparation, characterization,and pharmacokinetic pro?le in mice.J Liposome Res 2011;21(3):237–44.
J.Wang et al./Engineering5(2019)32–3939
Engineering 2 (2016) xxx–xxx
Research
Traditional Chinese Medicine—Review
青蒿素——一种从中药中发现的神奇药物
王继刚a ,b ,c ,#, 徐承超c ,#, 王彦钧d ,#, 李玉洁a ,b , 廖福龙a ,b , 姜廷良a ,b , 屠呦呦a ,b ,*
a Artemisinin Research Center, China Academy of Chinese Medical Sciences, Beijing 100700, China
b
Institute of Chinese Materia Medica, China Academy of Chinese Medical Sciences, Beijing 100700, China c
Department of Pharmacology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore 117600, Singapore d
Department of Physiology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore 117597, Singapore
a r t i c l e i n f o
摘要
Article history:
Received 8 June 2018Revised 1 August 2018
Accepted 12 November 2018
Available online 18 December 2018
青蒿素及其衍生物是治疗疟疾最重要且最具影响力的一类药物。自20 世纪70 年代初发现青蒿素以来,国际上在研究这种非凡的植物化学药物及探明其独特的化学和药理特性方面取得了巨大进展。现今,虽然青蒿素及其衍生物仍然是抗疟的支柱药物,但它们的持续应用和发展也面临许多挑战,包括青蒿素治疗疟疾过程中出现的耐药现象以及青蒿素在其他疾病中的应用。在本文中,我们描述了青蒿素类药物的早期发现、发展过程、应用现状以及未来的发展前景。另外,我们总结了当前的青蒿素机制研究情况并提出了一些看法,同时强调了机制研究对于青蒿素类药物在抗疟以及其他疾病治疗中的重要性。
? 2018 THE AUTHORS. Published by Elsevier LTD on behalf of Chinese Academy of Engineering and Higher
Education Press Limited Company This is an open access article under the CC BY-NC-ND license
关键词青蒿
作用机制疟疾抗癌
1.引言
疟疾自古以来就是一种具有全球影响的衰竭性疾病,至今仍是传播最广泛和最具破坏性的传染病之一[1]。长期以来,疟疾的病因被错误地归咎于“恶劣的空气”,直到19世纪末Charles Louis Alphonse Lave-ran 和Ronald Ross 的著作问世,人们才知道疟疾具有传染性和寄生性。他们发现疟原虫属原生动物是导致疟疾的罪魁祸首,按蚊是疟疾感染的主要媒介。这些发现使Laveran 和Ross 成为了诺贝尔生理学或医学奖的最早获得者[2]。
在这些发现问世之后的几十年里,疟疾的治疗取得
了突破性进展。20世纪60年代末,中国政府组织了一项旨在寻找抗疟药物的研究,并最终发现了青蒿素。青蒿素(及其衍生物,本文中我们将其称为“青蒿素”)是一种具有独特化学结构的倍半萜烯内酯化合物(图1),来源于紫草属植物黄花蒿(Artemisia annua L.,图2)。自发现以来,它已成为最重要和最有效的抗疟药物[3]。
从很多方面看,青蒿素都是一种令人真正着迷的药物。青蒿素传奇的发现过程(从传统药物中筛选和提取的复杂过程)及作为抗疟药物的卓越效力和影响力使它一登上世界舞台就受到了极大的关注[1]。在被发现40多年后,青蒿素仍然是主要抗疟治疗的基础[4]。多年来人们在青蒿素作用机制的研究上做了很多工作[5]。
* Corresponding author.
E-mail address:
yytu@https://www.doczj.com/doc/8513572562.html, (Y. Tu)
Contents lists available at ScienceDirect
Engineering
36Author name et al. / Engineering 2(2016) xxx–xxx
除此之外,人们还发现青蒿素具有除抗疟活性以外的其他药理作用,使人们对它的发展充满了期待[6]。
鉴于此,我们认为现在应该对这一具有影响力的药物的过去、现在和未来做一个总结。本文回顾了青蒿素的发现和发展历程,总结了当前对于青蒿素在抗疟中的作用机制研究情况,并展望了青蒿素在其他方面的应用前景。本文将对青蒿素做出一个全面的介绍,并基于青蒿素的研究现状发表观点。
2.青蒿素的发现
首先我们将简要回顾青蒿素发现和发展的非凡历程。中医关于疟疾的记载可以追溯到几千年前,而青蒿作为药材的使用也是如此。首次提到青蒿用于疟疾治疗可以追溯到东晋(公元317—420年)葛洪的《肘后备急
方》,随后青蒿和其他技术在疟疾防治中的应用在中国一系列历史医学著作中常有记载,其中包括颇具影响力的李时珍的《本草纲目》(明代,公元1368—1644年)。这些丰富的古代记载对于青蒿素的发现和发展做出了巨大贡献。
在第二次世界大战之后的几年里,强力杀虫剂二氯二苯三氯乙烷(DDT )和氯喹(CQ )等新型抗疟药物的研制和部署使疟疾防治工作取得了巨大进展。然而,世界卫生组织(WTO )在20世纪50年代在世界各地抗击和根除疟疾的运动中遇到了与耐药性相关的挑战。DTT 耐药载体和耐药寄生虫的出现导致了疟疾的再次爆发,在东南亚和撒哈拉以南非洲地区尤为严重[7]。人们对于新型抗疟药物的需求变得十分迫切。由于越南战争和该地区耐药疟原虫的流行,美国也投入了大量财力研发新型抗疟药物。在此期间,中国政府也开始了抗疟研究工作。中国政府设立了一个名为“523”(以其1967
年5月23日启用之日命名)的国家项目,以便在国家级水平上加强抗疟药物的研究[8]。
1969年,屠呦呦教授被选为该项目的研究组组长,该研究组致力于在中药中筛选抗疟新药。这项研究是在中国中医科学院中药研究所进行的。屠呦呦和她的同事从大量的中医知识宝库(包括古代文学、民间传说和中医从业者的口头采访)中初步选择了2000多种草药,其中640种被认为是可能有效的中草药,并从其中的200多种草药(包括青蒿/青蒿提取物)中提取了380多种提取物进行测试,大多数结果都不令人满意[1,9]。然而,在1971年,青蒿的提取物引起了他们的特别关注,因为它产生了理想但不稳定的抑制率[1]。这一发现促使他们对文献进行了修正,这可能是发现青蒿素过程中最重要的突破。
回到葛洪的《肘后备急方》这一最早使用青蒿治疗疟疾症状的著作,屠呦呦注意到,青蒿的使用方法是使用浸泡青蒿的水,即青蒿的“汁液”。值得注意的是,书中并没有提到中医处方中很常见的药物加热过程。屠
图1.
青蒿素及其临床应用衍生物。
图2. 田间的黄花蒿。
37 Author name et al. / Engineering 2(2016) xxx–xxx
呦呦从文献资料和自己对中医的了解中提出了低温条件提取有效成分的想法。通过分离酸性和中性相进一步纯化提取液,以保留活性成分,同时降低原提取液的毒性。在1971年10月前后进行的实验中,该物质对鼠类疟疾显示出了100%的惊人疗效。这一显著结果在同年12月底的猴疟疾实验中得到了重现,从而毫无疑问地确认了青蒿提取物的有效性[1]。
虽然已经取得突破性进展,但药物开发的征程还远未完成。当时中国的情况导致新药临床试验难以开展,无法确定其对人体是否安全有效。由于疟疾研究具有季节性和时间敏感性,为了加快这一进程,屠呦呦及其同事决定自愿成为第一批进行毒性和剂量探索试验的受试者[8]。这一试验确认了青蒿提取物对人体的安全性,并使更大规模的临床试验能够在1972年下半年顺利进行。这些临床试验在海南省和北京的中国人民解放军302医院(现并入中国人民解放军总医院第五医学中心)开展,证明了青蒿素的成功,并为将青蒿素的研究推向国家水平铺平了道路。此后,中国科学界的共同努力推动了青蒿的进一步研究和发展。1972年11月,屠呦呦所在的中药研究所团队从青蒿中分离出活性成分青蒿素。随后,该团队又开发了二氢青蒿素(DHA),其仍然是当今最具药理学活性的青蒿素衍生物之一。在随后的10年里,屠呦呦研究团队与全国其他研究所合作,进一步开展了一系列药物开发的基础工作,包括确定青蒿素的立体结构并开发更多的青蒿素衍生物[10,11]。1981年在北京举行的疟疾化学治疗科学工作组第四次会议上,屠呦呦首次公布这些研究成果而使青蒿素的研究达到高潮。该研究小组即中国青蒿合作课题组在1982年发表了一系列青蒿素及其衍生物的抗疟相关论文[12,13]。因此,青蒿素成为了传统中医药送给世界人类的礼物。
在随后的20世纪80年代,青蒿素及其衍生物在中国成功地治愈了成千上万的疟疾患者[1]。不久之后亚洲其他疟疾流行地区也开始使用青蒿素进行临床治疗[14–19]。令人鼓舞的治疗效果使得青蒿素治疗疟疾的方法迅速传播,尤其是在非洲地区[19–24]。有证据表明,以青蒿素为基础的治疗,特别是与作用较慢的抗疟药如甲氟喹或哌喹联合使用,可显著促进寄生虫的清除,并迅速改善恶性疟原虫(Plasmodium falciparum)感染的症状。与此同时,青蒿素对于耐药疟原虫的治疗作用也十分显著,且关于毒性和安全问题的报道很少[25]。经过十多年的独立随机临床研究和统计分析,青蒿素类药物的疗效和安全性越发明晰。最后,在2006年,WTO
宣布改变其治疗疟疾的战略,充分利用青蒿素联合疗法(ACT)作为治疗疟疾的一线疗法[26]。目前,ACT仍然是最有效和最推荐的抗疟疗法[4]。
3. 青蒿素的作用机制研究
自ACT成为疟疾的官方一线治疗手段至今已经十多年了,距青蒿素的发现也有三十多年的时间。在此期间,人们对青蒿素治疗的临床和药理特征进行了广泛的研究和报道[27–30]。尽管各种青蒿素衍生物的具体特性可能不同,但它们都具有作用迅速、效力高、毒性低、半衰期短等共同特性,这使得青蒿素类药物和长效抗疟药物的联合治疗成为理想和推荐的抗疟疗法[30]。除了其药理学性质外,阐明药物的作用机制对优化治疗方案也非常重要。剂量、药物组合甚至耐药性都与药物活性的分子机制密切相关。然而,尽管经历了数十年的广泛应用,我们对青蒿素作用机制的了解仍然相当不全面,这多少有些令人惊讶。在此,我们简要概述了目前对青蒿素的主流认识以及青蒿素机制研究的最新进展[31,32]。总的来说,青蒿素的显著治疗特性可以认为是两方面的特点导致的:其独特的激活机制以及其下游的药物靶点。这些机制结合在一起,产生了一种效力高且特异性强的药物。
3.1. 药物的激活
青蒿素及其衍生物是倍半萜内酯,其药效团为1,2,4-三氧杂环已烷[33]。这个基团中的过氧化桥结构对青蒿素的药理活性至关重要[13,34,35]。青蒿素从两种意义上看是一种前药:一是许多衍生物在体内被迅速转化为二氢青蒿素;二是它们的药理作用依赖于过氧化桥结构的断裂,这种断裂机制仍是目前研究的热点之一[36]。疟原虫的特征是在其生命周期的红细胞阶段广泛摄取和消化血红蛋白[37,38],从而释放了大量游离的具有还原活性的血红素和亚铁离子(Fe2+),这被认为是青蒿素特异性杀伤寄生虫的基础。事实上,血红蛋白的消化与寄生虫对青蒿素的敏感性密切相关[38,39]。对于过氧化桥的断裂是由活性血红素还是游离的亚铁离子激活的,以及断裂后下游的分子作用机制,人们提出了多种模型[36,40–48]。这些模型在过氧桥断裂的本质和药物激活产生的反应中间体的特性方面有所不同。然而,总的来说,它们解释了药物在产生活性物质的寄生虫中特异性激活,从而导致细胞损伤和寄生虫死亡。最近的证据表
38Author name et al. / Engineering 2(2016) xxx–xxx
明,游离的氧化还原活性血红素可能在青蒿素激活中起主导作用[49,50]。2008年的一项体外研究表明,与血红素、游离亚铁和未消化血红蛋白等其他含铁物质相比,亚铁血红素可能是一种更强的青蒿素激活剂[49]。在寄生虫中也进行了类似的观察,抑制血红蛋白消化可以阻断青蒿素的活化,而鳌合游离的亚铁离子无此效应[47]。因此,在感染的红细胞中消化血红蛋白的过程是疟原虫生长所必需的,是青蒿素特异性激活的关键[38]。
有趣的是,周兵课题组在以酵母为研究体系的研究[51,52]中发现线粒体可直接参与青蒿素的激活和药理作用,从而进一步将青蒿素的作用机制与活性氧类(ROS)的产生和氧化损伤联系起来。在不同环境或区域可能存在不同的青蒿素激活方式,这些环境或区域的激活条件和激活幅度可能不同[53]。在以后的研究中,必须考虑药物激活在青蒿素活性中的关键作用,并进一步阐明其在不同条件下的作用机制。
3.2. 下游机制
确定细胞靶点是阐明药物作用机制的关键步骤。人们对药物设计及其作用机制的传统理解是药物通过修饰一个或多个特定的细胞靶标,如蛋白质,从而对下游通路产生影响。然而,青蒿素快速、有效和使靶标蛋白烷基化的特性,可能源自于另一种完全不同的作用机制。
首先,如前文所述,血红素能够从药物激活途径之外的血红蛋白消化中释放。过量的血红素在受感染的红细胞中转化为高铁血红素,其能够通过氧化损伤和直接裂解细胞膜的方式发挥抗寄生虫毒性[54]。因此,疟原虫进化出了一种解毒机制,可以通过生物结晶过程将血红蛋白转化为无毒的、惰性的结晶疟原虫素[55]。据报道,活化的青蒿素能够通过血红素的烷基化反应阻止疟原虫素的形成,这与其他抗疟药物的药效机制相仿,如CQ[45,56–58]。因此,血红蛋白消化过程中的游离血红素既是青蒿素的激活剂又是其作用靶点[45]。
考虑到活化的青蒿素可以产生ROS,因此,也有报道称青蒿素可以直接对靶标蛋白进行烷基化修饰[59,60]。转译控制肿瘤蛋白(TCTP)和肌浆内质网Ca2+-ATP酶(PfATP6)被证实是青蒿素类药物激活后的作用靶标[61–63]。青蒿素的作用机制已由针对单个靶点的研究演变为针对潜在的多个靶标的研究[64–67]。利用蛋白质组学方法,已经观察到青蒿素的靶标可能是混杂的,而不是单一的。在首例系统报道青蒿素结合靶标的研究中,研究工作者在活的疟原虫株中筛选并鉴定了100多种青蒿素靶点蛋白[47]。而在Ismail等[68]的研究中也得出了类似的结论。这些结果证实了青蒿素从激活到烷基化抑制多种蛋白活性,进而扰乱多种关键的生物功能,最终发挥寄生虫毒性的复杂机制[47,48,50]。有趣的是,PfATP6和其他关键转运蛋白如PfCRT和Pfmdr1在这类实验中均被标记。这与前期发现PfATP6是青蒿素的重要靶标结果相互印证[47,68]。此外,青蒿素与TCTP的结合位点的确定进一步支持了血红素激活的复杂机制,其修饰位点邻近且本质上是随机的[50]。
基于对青蒿素已有的认知,我们已可以清楚地描述青蒿素的作用机制。青蒿素及其衍生物是一种前药,过氧桥的裂解是其激活和发挥抗疟活性所必需的关键步骤。青蒿素的激活过程依赖于受感染的红细胞所特有的、同时也是寄生虫代谢不可或缺的富含血红素的环境。而后,活化的青蒿素利用富含血红素的环境有效地杀死寄生虫。这种药效机制将红细胞的感染、寄生虫的生长与药物激活联系在一起,从而为青蒿素的治疗提供了显著的特异性和低毒性。另一方面,活化的青蒿素也在无选择性地破坏相邻蛋白活性和细胞结构。与大多数传统药物(包括大多数抗疟药)不同,青蒿素的作用靶标不是单一蛋白质或细胞功能,而是像一颗“炸弹”,在激活后引爆,造成广泛性的损害。因此,可以认为青蒿素的特异性是基于其活性而不是其靶点。青蒿素的这些特性使其成为对抗疟疾的最理想武器,特别是和其他机制迥异却能与青蒿素产生互补作用的药物联合使用时。多重靶标药物的另一个明显优势是不易形成耐药性,原因是少数靶标的突变不足以对药物活性产生严重影响。这一优势也很好地解释了青蒿素在长达几十年的广泛应用中仍能保持药物活性的原因。
然而,ACT清除疟疾的速度正在逐渐放缓,特别是在亚洲疟疾流行地区,疟疾的发病率也有上升的趋势[69]。近期的评论从多个角度对这一问题进行了全面的论述[69–75]。尽管领域内对“青蒿素耐药性”的确切定义存在争议,但鉴于青蒿素在疟疾控制中所占的地位,这种威胁无疑是切实存在的[76,77]。要解决这个燃眉之急,必须克服两大挑战:①必须充分了解青蒿素的作用机制;②必须确定新出现的耐青蒿素疟原虫株的遗传和生理特征。尽管近年来人们的研究成果已基本揭开了青蒿素作用机制的神秘面纱,但青蒿素耐药性疟原虫的分子特征仍然模糊不清。我们需要继续努力来全面了解青蒿素耐药性与其作用机制之间的关系,并基于这些新知识开发和测试新的治疗策略。
39 Author name et al. / Engineering 2(2016) xxx–xxx
4. 青蒿素的其他药理活性
青蒿素疗法具有患者耐受性良好和价格低廉的特点,这使青蒿素成为一种特别值得开发其新功能的药物。事实上,自从青蒿素首次被世界所知以来,人们对青蒿素抗疟活性以外的药理作用的研究兴趣一直在稳步增长[78]。虽然疟疾仍然是青蒿素被批准治疗的唯一疾病,但多年来,人们认真探索了青蒿素在抗癌、抗炎、抗寄生虫(疟疾之外)和抗病毒等方面的药理活性[78–82]。在此,我们简要地总结了一些青蒿素在其他疾病领域的研究成果,特别是在癌症治疗领域,用以作为未来药物研发的一扇窗口。
1993年,人们首次研究报道了青蒿素在癌症治疗中的作用,此后青蒿素的抗癌作用得到了广泛的研究和推广[83–85]。目前,大量研究结果表明青蒿素及其衍生物对体外和体内多种类型癌症表现出了选择性的细胞毒性[86],有希望进行小规模的临床试验[87–89]。在对青蒿素抗癌作用进行了20多年的研究后,研究人员发现了大量潜在的抗癌靶标和作用机制。据报道,青蒿素能诱导线粒体凋亡和其他形式的癌细胞凋亡,如导致坏死、抑制肿瘤转移血管新生、阻滞癌细胞周期等[90–97]。报道称这些结果与氧化损伤、DNA损伤、基因表达突变以及哺乳动物雷帕霉素靶蛋白(mTOR)、NF-κB、促分裂原活化蛋白质(MAP)激酶、Wnt/β-catenin等多种信号通路的相互作用息息相关[82,98–102]。这些途径和作用机制在最近的研究成果中得到了广泛的论述[79–82]。
虽然通路验证是药物作用机制研究的一个重要方面,但也有必要像人们在青蒿素的抗疟研究中所做的一样考虑将药物的激活和下游活性统一起来。青蒿素在抗癌作用中的激活机制很可能与其在抗疟作用中的类似,并且可能与其药效作用的特异性密切相关。因此,游离亚铁与游离血红素的作用再次受到人们的重视,尤其是考虑到铁与青蒿素诱导的癌症细胞毒性密切相关[103,104]。最近的研究进一步阐明了血红素能够对癌细胞中的青蒿素发挥激活作用。特别是人们利用一系列的方法证明了血红素合成及活性与青蒿素的细胞毒性显著相关[105–108]。同样值得注意的是,报道称癌细胞具有更高的血红素代谢和合成水平,表明青蒿素可能以类似抗疟的作用方式巩固其抗癌作用的特异性[109–111]。青蒿素与线粒体(哺乳动物细胞血红素合成的细胞器)的特异性靶向结合或通过血红素前体氨基乙酰丙酸(ALA)处理提高血红素水平,都能够使其抗癌活性显著升高[112–114]。以血红素为中心的激活机制和铁依赖性的下游细胞毒性机制可能是青蒿素抗癌活性中作用的调和点[115]。进一步深入了解青蒿素在癌症中特异性的机制对未来的应用至关重要。
另一方面,在进一步验证青蒿素抗癌作用机制时,有必要考虑适当的方向。以疟疾为例,在发挥抗疟作用时,青蒿素被激活后无差别地攻击邻近目标。如果青蒿素在癌细胞中以类似的方式被激活,那么多靶点机制可能也会发生。这将解释已经报道的青蒿素的不同细胞效应和多个相关途径,因为多个靶点和功能途径可能同时受到复杂机制的影响。事实上,最近使用蛋白质组学方法对青蒿素抗癌靶点进行的研究揭示了青蒿素在癌细胞中的多靶点机制[48,113,114]。细胞毒性机制本身也是一个非常重要的问题,尤其是对于非凋亡的细胞死亡形式。最近的研究将青蒿素诱导的细胞毒性与氧化损伤和溶酶体功能紧密联系在一起,重点关注铁在导致铁依赖型细胞死亡(细胞铁死亡)中的作用[116–118]。特别是溶酶体介导的自噬条件下的铁蛋白降解(称为铁蛋白吞噬作用)释放出的游离亚铁,从而导致细胞铁死亡和铁介导的ROS生成[93,119]。据报道,自噬是一种能够被青蒿素激活的细胞过程,但对癌细胞存活和细胞毒性的影响尚不明确[115,119]。显然,自噬、溶酶体活性、游离亚铁和铁依赖性的细胞铁死亡之间的关系是青蒿素抗癌机制研究中主要的未知领域。寻找新的癌症特异性靶标和阐明抗癌作用机制的研究正在稳步进行,并将继续推动青蒿素成为一种抗癌药物。最近的报道揭示了青蒿素介导的对癌症干细胞、免疫调节、肿瘤转移、包括糖酵解调节在内的癌症代谢以及信号传导途径(包括STAT3、NF-κB、mTOR和CREBP等)的影响,并为进一步验证指明了新的方向[115,120,121]。另外,鉴于免疫调节药物在癌症治疗中的复杂作用,青蒿素通过调节T细胞(Treg)活性和产生如前列腺素E2(PGE2)在内的免疫抑制性细胞因子从而发挥免疫调节作用的潜在能力值得注意[122–125]。最后,一些为改进以青蒿素为基础的药物的配方和递送方式的尝试,为提高青蒿素疗效和降低其耐药性开拓了光明的前景。这些研究成果包括新的合成二聚体、三聚体和药物结合物(尤其是转铁蛋白结合系统)以及联合治疗,这个全新的青蒿素研究领域在最近的报道中得到了充分的讨论[126–135]。
除了抗癌活性,青蒿素在治疗其他疾病方面的潜力也在被广泛研究。特别是针对自身免疫性疾病和过敏性哮喘等的抗炎作用已在一系列疾病模型中得到验
40Author name et al. / Engineering 2(2016) xxx–xxx
证[78]。其中一些实验结果与接受青蒿素治疗的疟疾患者免疫抑制的观察结果相关[136]。青蒿素对疱疹、乙型和丙型肝炎病毒表现出了较强的抗病毒作用,并且对包括血吸虫病在内的其他寄生虫病表现出治疗作用[137–141]。最近的研究还发现了一种值得注意的争议现象:青蒿素在糖尿病模型中能将胰岛α细胞诱导转化为胰岛β细胞[142,143]。这些药理作用机制主要集中在ROS的生成和氧化损伤诱导的内过氧化物裂解,此外,也有人提出了一些其他的作用机制(包括不依赖于内过氧化物的),尤其是在免疫激活的情况下[78,144]。在考虑药物活化条件的重要性的同时,必须清楚地了解药物的作用机制和在不同应用条件下功能的区别。同样值得注意的是,为了避免可能的干扰或并发症,最好在没有罹患疟疾或无感染疟疾风险的患者和地区中进行青蒿素其他药理活性的研究。必须尽一切努力确保在不损害当前应用的前提下充分发挥青蒿素的潜力。
5. 结论
青蒿素类药物给世界抗疟事业带来了曙光。青蒿素的有效性、安全性和廉价性使其成为抗疟疾的一线药物,已挽救了数以百万的生命。自从青蒿素被发现以来,国际社会的共同努力已经使其成为最理想的抗疟药物。其他领域的研究成果也表明,青蒿素在抗疟之外也具有广泛的应用前景。我们认为,在一定能力范围内寻求青蒿素的效用最大化是合理的。在青蒿素的抗疟研究中,一方面应当继续阐明青蒿素的激活和作用机制,另一方面应进一步提高其单独或联合用药时的药理活性[145]。加强对青蒿素作用机制的理解是阐明青蒿素耐药性机制的关键。这些努力将确保青蒿素在既往优势领域继续发挥类似甚至更大的作用。展望未来,建立在人们对疾病作用机制深入了解基础上的青蒿素再利用研究,必将推动青蒿素的未来发展。最后,我们衷心希望青蒿素这一来自传统中医药的礼物能够在未来的许多年里继续为全世界人民的健康事业服务。
致谢
感谢资助本文工作的国家自然科学基金(项目编号:81641002和 81473548);国家科技重大专项重大新药创制(项目编号:2017ZX09101002-001-001-05和2017ZX09101002-001-001-03);中央级公益性研究院所基本科研业务费(项目编号:ZZ10-024 和ZXKT18003)。感谢陈利娜、向丽和师玉华博士提供的黄花蒿图片。感谢Sanjeev Krishna和Svetlana Tsogoeva 教授对本文提出的宝贵意见和帮助。
Compliance with ethics guidelines
Jigang Wang, Chengchao Xu, Yin Kwan Wong, Yujie Li, Fulong Liao, Tingliang Jiang, and Youyou Tu declare that they have no conflict of interest or financial conflicts to disclose.
References
[1] Tu Y. Artemisinin—a gift from traditional Chinese medicine to the world
(Nobel lecture). Angew Chem Int Ed 2016;55(35):10210–26.
[2] Cox FE. History of the discovery of the malaria parasites and their vectors.
Parasit Vectors 2010;3(1):5.
[3] Krishna S, Bustamante L, Haynes RK, Staines HM. Artemisinins: their growing
importance in medicine. Trends Pharmacol Sci 2008;29(10):520–7.
[4] World Health Organization. World malaria report 2017. Geneva: World
Health Organization; 2017.
[5] Ding XC, Beck HP, Raso G. Plasmodium sensitivity to artemisinins: magic
bullets hit elusive targets. Trends Parasitol 2011;27(2):73–81.
[6] Efferth T, Romero MR, Bilia AR, Osman AG, Sohly ME, et al. Expanding the
therapeutic spectrum of artemisinin: activity against infectious diseases beyond malaria and novel pharmaceutical developments. World J Tradit Chin Med 2016;2(2):1–23.
[7] D’Alessandro U, Butti?ns H. History and importance of antimalarial drug
resistance. Trop Med Int Health 2001;6(11):845–8.
[8] Tu Y. The discovery of artemisinin (Qinghaosu) and gifts from Chinese
medicine. Nat Med 2011;17(10):1217–20.
[9] Liao F. Discovery of artemisinin (Qinghaosu). Molecules 2009;14(12):5362–6.
[10] Collaboration Research Group for Qinghaosu. A new sesquiterpene lactone—
Qinghaosu. Chin Sci Bull 1997;3:142. Chinese.
[11] Wang MY. Publication process involving the discovery of artemisinin
(Qinghaosu) before 1985. Asian Pac J Trop Biomed 2016;6(6):461–7.
[12] China Cooperative Research Group on Qinghaosu and Its Derivatives as
Antimalarials. Chemical studies on Qinghaosu (artemisinine). J Tradit Chin Med 1982;2(1):3–8. Chinese.
[13] Klayman DL. Qinghaosu (artemisinin): an antimalarial drug from China.
Science 1985;228(4703):1049–55.
[14] Jiang JB, Li GQ, Guo XB, Kong YC, Arnold K. Antimalarial activity of mefloquine
and Qinghaosu. Lancet 1982;2(8293):285–8.
[15] Looareesuwan S, Viravan C, Vanijanonta S, Wilairatana P, Suntharasamai P,
Charoenlarp P, et al. Randomised trial of artesunate and mefloquine alone and in sequence for acute uncomplicated falciparum malaria. Lancet 1992;339 (8797):821–4.
[16] N o s t e n F,L u x e m b u r g e r C,t e r K u i l e F O,Wo o d r o w C,E h J P,
Chongsuphajaisiddhi T, et al. Treatment of multidrug-resistant Plasmodium falciparum malaria with 3-day artesunate-mefloquine combination. J Infect Dis 1994;170(4):971–7.
[17] Tran TH, Day NP, Nguyen HP, Nguyen TH, Tran TH, Pham PL, et al. A controlled
trial of artemether or quinine in Vietnamese adults with severe falciparum malaria. N Engl J Med 1996;335(2):76–83.
[18] Looareesuwan S, Wilairatana P, Viravan C, Vanijanonta S, Pitisuttithum P,
Kyle DE. Open randomized trial of oral artemether alone and a sequential combination with mefloquine for acute uncomplicated falciparum malaria.
Am J Trop Med Hyg 1997;56(6):613–7.
[19] Adjuik M, Babiker A, G arner P, Olliaro P, Taylor W, White N, et al;
International Artemisinin Study G roup. Artesunate combinations for treatment of malaria: meta-analysis. Lancet 2004;363(9402):9–17.
[20] Von Seidlein L, Jaffar S, Pinder M, Haywood M, Snounou G, Gemperli B, et al.
Treatment of African children with uncomplicated falciparum malaria with a new antimalarial drug, CGP 56697. J Infect Dis 1997;176(4):1113–6.
[21] Von Seidlein L, Bojang K, Jones P, Jaffar S, Pinder M, Obaro S, et al. A
randomized controlled trial of artemether/benflumetol, a new antimalarial and pyrimethamine/sulfadoxine in the treatment of uncomplicated falciparum malaria in African children. Am J Trop Med Hyg 1998;58
(5):638–44.
41 Author name et al. / Engineering 2(2016) xxx–xxx
[22] Doherty JF, Sadiq AD, Bayo L, Alloueche A, Olliaro P, Milligan P, et al. A
randomized safety and tolerability trial of artesunate plus sulfadoxine— pyrimethamine versus sulfadoxine-pyrimethamine alone for the treatment of uncomplicated malaria in Gambian children. Trans R Soc Trop Med Hyg 1999;93(5):543–6.
[23] Dondorp AM, Fanello CI, Hendriksen IC, Gomes E, Seni A, Chhaganlal KD, et al;
AQUAMAT Group. Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial. Lancet 2010;376(9753):1647–57.
[24] WWARN Artemisinin based Combination Therapy (ACT) Africa Baseline
Study Group. Clinical determinants of early parasitological response to ACTs in African patients with uncomplicated falciparum malaria: a literature review and meta-analysis of individual patient data. BMC Med 2015;13:212.
[25] Efferth T, Kaina B. Toxicity of the antimalarial artemisinin and its derivatives.
Crit Rev Toxicol 2010;40(5):405–21.
[26] Wo rl d H e a l t h O r g a n i z a t i o n.G u i d e l i n e s f o r t h e t re a t m e n t o f
malaria. Geneva: World Health Organization; 2006.
[27] Luo XD, Shen CC. The chemistry, pharmacology, and clinical applications of
Qinghaosu (artemisinin) and its derivatives. Med Res Rev 1987;7(1):29–52. [28] White NJ. Clinical pharmacokinetics and pharmacodynamics of artemisinin
and derivatives. Trans R Soc Trop Med Hyg 1994;88(Suppl 1):S41–3.
[29] De Vries PJ, Dien TK. Clinical pharmacology and therapeutic potential of
artemisinin and its derivatives in the treatment of malaria. Drugs 1996;52
(6):818–36.
[30] G erman PI, Aweeka FT. Clinical pharmacology of artemisinin-based
combination therapies. Clin Pharmacokinet 2008;47(2):91–102.
[31] Robert A, Dechy-Cabaret O, Cazelles J, Meunier B. From mechanistic studies
on artemisinin derivatives to new modular antimalarial drugs. Acc Chem Res 2002;35(3):167–74.
[32] Li J, Zhou B. Biological actions of artemisinin: insights from medicinal
chemistry studies. Molecules 2010;15(8):1378–97.
[33] Van Agtmael MA, Eggelte TA, van Boxtel CJ. Artemisinin drugs in the
treatment of malaria: from medicinal herb to registered medication. Trends Pharmacol Sci 1999;20(5):199–205.
[34] Meshnick SR, Taylor TE, Kamchonwongpaisan S. Artemisinin and the
antimalarial endoperoxides: from herbal remedy to targeted chemotherapy.
Microbiol Rev 1996;60(2):301–15.
[35] Posner GH, O’Neill PM. Knowledge of the proposed chemical mechanism of
action and cytochrome p450 metabolism of antimalarial trioxanes like artemisinin allows rational design of new antimalarial peroxides. Acc Chem Res 2004;37(6):397–404.
[36] O’Neill PM, Barton VE, Ward SA. The molecular mechanism of action of
artemisinin—the debate continues. Molecules 2010;15(3):1705–21.
[37] Lew VL, Tiffert T, Ginsburg H. Excess hemoglobin digestion and the osmotic
stability of Plasmodium falciparum-infected red blood cells. Blood 2003;101
(10):4189–94.
[38] Klonis N, Crespo-Ortiz MP, Bottova I, Abu-Bakar N, Kenny S, Rosenthal PJ,
et al. Artemisinin activity against Plasmodium falciparum requires hemoglobin uptake and digestion. Proc Natl Acad Sci USA 2011;108(28):11405–10.
[39] Xie SC, Dogovski C, Hanssen E, Chiu F, Yang T, Crespo MP, et al. Haemoglobin
degradation underpins the sensitivity of early ring stage Plasmodium falciparum to artemisinins. J Cell Sci 2016;129(2):406–16.
[40] Zhang F, Gosser DK Jr, Meshnick SR. Hemin-catalyzed decomposition of
artemisinin (Qinghaosu). Biochem Pharmacol 1992;43(8):1805–9.
[41] Posner GH, Oh CH, Wang D, Gerena L, Milhous WK, Meshnick SR, et al.
Mechanism-based design, synthesis, and in vitro antimalarial testing of new 4-methylated trioxanes structurally related to artemisinin: the importance of
a carbon-centered radical for antimalarial activity. J Med Chem 1994;37
(9):1256–8.
[42] Wu WM, Wu Y, Wu YL, Yao ZJ, Zhou CM, Li Y, et al. Unified mechanistic
framework for the Fe(II)-induced cleavage of Qinghaosu and derivatives/ analogues. The first spin-trapping evidence for the previously postulated secondary C-4 radical. J Am Chem Soc 1998;120(14):3316–25.
[43] Stocks PA, Bray PG, Barton VE, Al-Helal M, Jones M, Araujo NC, et al. Evidence
for a common non-heme chelatable-iron-dependent activation mechanism for semisynthetic and synthetic endoperoxide antimalarial drugs. Angew Chem Int Ed 2007;46(33):6278–83.
[44] Haynes RK, Chan WC, Lung CM, Uhlemann AC, Eckstein U, Taramelli D, et al.
The Fe2+-mediated decomposition, PfATP6 binding, and antimalarial activities of artemisone and other artemisinins: the unlikelihood of C-centered radicals as bioactive intermediates. ChemMedChem 2007;2(10):1480–97.
[45] Meunier B, Robert A. Heme as trigger and target for trioxane-containing
antimalarial drugs. Acc Chem Res 2010;43(11):1444–51.
[46] Haynes RK, Cheu KW, N’Da D, Coghi P, Monti D. Considerations on the
mechanism of action of artemisinin antimalarials: part 1—the ‘carbon radical’ and ‘heme’ hypotheses. Infect Disord Drug Targets 2013;13(4):217–77.
[47] Wang J, Zhang CJ, Chia WN, Loh CC, Li Z, Lee YM, et al. Haem-activated
promiscuous targeting of artemisinin in Plasmodium falciparum. Nat Commun 2015;6:10111.
[48] Zhou Y, Li W, Xiao Y. Profiling of multiple targets of artemisinin activated by
hemin in cancer cell proteome. ACS Chem Biol 2016;11(4):882–8.
[49] Zhang S, Gerhard GS. Heme activates artemisinin more efficiently than
hemin, inorganic iron, or hemoglobin. Bioorg Med Chem 2008;16
(16):7853–61.[50] Li W, Zhou Y, Tang G, Xiao Y. Characterization of the artemisinin binding site
for translationally controlled tumor protein (TCTP) by bioorthogonal click chemistry. Bioconjug Chem 2016;27(12):2828–33.
[51] Li W, Mo W, Shen D, Sun L, Wang J, Lu S, et al. Yeast model uncovers dual roles
of mitochondria in action of artemisinin. PLoS Genet 2005;1(3):e36.
[52] Wang J, Huang L, Li J, Fan Q, Long Y, Li Y, et al. Artemisinin directly targets
malarial mitochondria through its specific mitochondrial activation. PLoS One 2010;5(3):e9582.
[53] Sun C, Li J, Cao Y, Long G, Zhou B. Two distinct and competitive pathways
confer the cellcidal actions of artemisinins. Microb Cell 2015;2(1):14–25. [54] Fitch CD, Chevli R, Kanjananggulpan P, Dutta P, Chevli K, Chou AC. Intracellular
ferriprotoporphyrin IX is a lytic agent. Blood 1983;62(6):1165–8.
[55] Egan TJ. Recent advances in understanding the mechanism of hemozoin
(malaria pigment) formation. J Inorg Biochem 2008;102(5–6):1288–99. [56] Cazelles J, Robert A, Meunier B. Alkylation of heme by artemisinin, an
antimalarial drug. Acad Sci Chem 2001;4(2):85–9.
[57] Robert A, Benoit-Vical F, Claparols C, Meunier B. The antimalarial drug
artemisinin alkylates heme in infected mice. Proc Natl Acad Sci USA 2005;102
(38):13676–80.
[58] Loup C, Lelièvre J, Benoit-Vical F, Meunier B. Trioxaquines and hemeartemisinin
adducts inhibit the in vitro formation of hemozoin better than chloroquine. Antimicrob Agents Chemother 2007;51(10):3768–70.
[59] Yang YZ, Little B. Meshnick SR. Alkylation of proteins by artemisinin. Effects
of heme, pH, and drug structure. Biochem Pharmacol 1994;48(3):569–73. [60] Meshnick SR. Artemisinin: mechanisms of action, resistance and toxicity. Int J
Parasitol 2002;32(13):1655–60.
[61] Bhisutthibhan J, Pan XQ, Hossler PA, Walker DJ, Yowell CA, Carlton J, et al. The
Plasmodium falciparum translationally controlled tumor protein homolog and its reaction with the antimalarial drug artemisinin. J Biol Chem 1998;273
(26):16192–8.
[62] Eckstein-Ludwig U, Webb RJ, Van Goethem ID, East JM, Lee AG, Kimura M,
et al. Artemisinins target the SERCA of Plasmod ium falciparum. Nature 2003;424(9651):957–61.
[63] Uhlemann AC, Cameron A, Eckstein-Ludwig U, Fischbarg J, Iserovich P, Zuniga
FA, et al. A single amino acid residue can determine the sensitivity of SERCAs to artemisinins. Nat Struct Mol Biol 2005;12(7):628–9.
[64] Krishna S, Pulcini S, Fatih F, Staines H. Artemisinins and the biological basis
for the PfATP6/SERCA hypothesis. Trends Parasitol 2010;26(11):517–23. [65] Arnou B, Montigny C, Morth JP, Nissen P, Jaxel C, M?ller JV, et al. The
Plasmodium falciparum Ca2+-ATPase PfATP6: insensitive to artemisinin, but a potential drug target. Biochem Soc Trans 2011;39(3):823–31.
[66] Cui L, Wang Z, Jiang H, Parker D, Wang H, Su XZ, et al. Lack of association of
the S769N mutation in Plasmod ium falciparum SERCA (PfATP6) with resistance to artemisinins. Antimicrob Agents Chemother 2012;56(5):2546–52.
[67] Krishna S, Pulcini S, Moore CM, Teo BH, Staines HM. Pumped up: reflections on
PfATP6 as the target for artemisinins. Trends Pharmacol Sci 2014;35(1):4–11. [68] Ismail HM, Barton V, Phanchana M, Charoensutthivarakul S, Wong MH,
Hemingway J, et al. Artemisinin activity-based probes identify multiple molecular targets within the asexual stage of the malaria parasites Plasmodium falciparum 3D7. Proc Natl Acad Sci USA 2016;113(8):2080–5. [69] Ashley EA, Dhorda M, Fairhurst RM, Amaratunga C, Lim P, Suon S, et al;
Tracking Resistance to Artemisinin Collaboration (TRAC). Spread of artemisinin resistance in Plasmodium falciparum malaria. N Eng J Med 2014;
371(5):411–23.
[70] Dondorp AM, Yeung S, White L, Nguon C, Day NP, Socheat D, et al. Artemisinin
resistance: current status and scenarios for containment. Nat Rev Microbiol 2010;8(4):272–80.
[71] Paloque L, Ramadani AP, Mercereau-Puijalon O, Augereau JM, Benoit-Vical F.
Plasmodium falciparum: multifaceted resistance to artemisinins. Malar J 2016;15:149.
[72] Tilley L, Straimer J, Gn?dig NF, Ralph SA, Fidock DA. Artemisinin action and
resistance in Plasmodium falciparum. Trends Parasitol 2016;32(9):682–96. [73] Wang J, Xu C, Lun ZR, Meshnick SR. Unpacking ‘artemisinin resistance’. Trends
Pharmacol Sci 2017;38(6):506–11.
[74] Gil JP, Krishna S. pfmdr1 (Plasmodium falciparum multidrug drug resistance
gene 1): a pivotal factor in malaria resistance to artemisinin combination therapies. Expert Rev Anti Infect Ther 2017;15(6):527–43.
[75] Hanscheid T, Hardisty DW. How ‘‘resistant” is artemisinin resistant
malaria?—The risks of ambiguity using the term ‘‘resistant” malaria. Travel Med Infect Dis 2018;24:23–4.
[76] Meshnick S. Perspective: artemisinin-resistant malaria and the wolf. Am J
Trop Med Hyg 2012;87(5):783–4.
[77] World Health Organization. Artemisinin and artemisinin-based combination
therapy resistance. Report. Geneva: World Health Organization; 2016 Apr. [78] Ho WE, Peh HY, Chan TK, Wong WS. Artemisinins: pharmacological actions
beyond anti-malarial. Pharmacol Ther 2014;142(1):126–39.
[79] Firestone GL, Sundar SN. Anticancer activities of artemisinin and its bioactive
derivatives. Expert Rev Mol Med 2009;11:e32.
[80] Crespo-Ortiz MP, Wei MQ. Antitumor activity of artemisinin and its
derivatives: from a well-known antimalarial agent to a potential anticancer drug. J Biomed Biotechnol 2012;2012:247597.
[81] Lai HC, Singh NP, Sasaki T. Development of artemisinin compounds for cancer
treatment. Invest New Drugs 2013;31(1):230–46.
[82] Efferth T. Artemisinin—second career as anticancer drug? World J Tradit Chin
Med 2015;1(4):2–25.
42Author name et al. / Engineering 2(2016) xxx–xxx
[83] Woerdenbag HJ, Moskal TA, Pras N, Malingré TM, el-Feraly FS, Kampinga HH,
et al. Cytotoxicity of artemisinin-related endoperoxides to Ehrlich ascites tumor cells. J Nat Prod 1993;56(6):849–56.
[84] Lai H, Singh NP. Selective cancer cell cytotoxicity from exposure to
dihydroartemisinin and holotransferrin. Cancer Lett 1995;91(1):41–6.
[85] Efferth T, Dunstan H, Sauerbrey A, Miyachi H, Chitambar CR. The anti-malarial
artesunate is also active against cancer. Int J Oncol 2001;18(4):767–73.
[86] Efferth T, Sauerbrey A, Olbrich A, Gebhart E, Rauch P, Weber HO, et al.
Molecular modes of action of artesunate in tumor cell lines. Mol Pharmacol 2003;64(2):382–94.
[87] Zhang ZY, Yu SQ, Miao LY, Huang XY, Zhang XP, Zhu YP, et al. Artesunate
combined with vinorelbine plus cisplatin in treatment of advanced non-small cell lung cancer: a randomized controlled trial. J Chin Integr Med 2008;6
(2):134–8.
[88] Jansen FH, Adoubi I, JC KC, DE Cnodder T, Jansen N, Tschulakow A, et al. First
study of oral Artenimol-R in advanced cervical cancer: clinical benefit, tolerability and tumor markers. Anticancer Res 2011;31(12):4417–22.
[89] Krishna S, Ganapathi S, Ster IC, Saeed ME, Cowan M, Finlayson C, et al. A
randomised, double blind, placebo-controlled pilot study of oral artesunate therapy for colorectal cancer. EBioMedicine 2014;2(1):82–90.
[90] Efferth T, Rücker G, Falkenberg M, Manns D, Olbrich A, Fabry U, et al.
Detection of apoptosis in KG-1a leukemic cells treated with investigational drugs. Arzneimittelforschung 1996;46(2):196–200.
[91] Willoughby JA Sr, Sundar SN, Cheung M, Tin AS, Modiano J, Firestone GL.
Artemisinin blocks prostate cancer growth and cell cycle progression by disrupting Sp1 interactions with the cyclin-dependent kinase-4 (CDK4) promoter and inhibiting CDK4 gene expression. J Biol Chem 2009;284
(4):2203–13.
[92] Steinbrück L, Pereira G, Efferth T. Effects of artesunate on cytokinesis and
G2/M cell cycle progression of tumour cells and budding yeast. Cancer Genomics Proteomics 2010;7(6):337–46.
[93] Hamacher-Brady A, Stein HA, Turschner S, Toegel I, Mora R, Jennewein N,
et al. Artesunate activates mitochondrial apoptosis in breast cancer cells via iron-catalyzed lysosomal reactive oxygen species production. J Biol Chem 2011;286(8):6587–601.
[94] Anfosso L, Efferth T, Albini A, Pfeffer U. Microarray expression profiles of
angiogenesis-related genes predict tumor cell response to artemisinins.
Pharmacogenomics J 2006;6(4):269–78.
[95] Button RW, Lin F, Ercolano E, Vincent JH, Hu B, Hanemann CO, et al.
Artesunate induces necrotic cell death in schwannoma cells. Cell Death Dis 2014;5:e1466.
[96] Buommino E, Baroni A, Canozo N, Petrazzuolo M, Nicoletti R, Vozza A, et al.
Artemisinin reduces human melanoma cell migration by down-regulating αVβ3 integrin and reducing metalloproteinase 2 production. Invest New Drugs 2009;27(5):412–8.
[97] Chen T, Li M, Zhang R, Wang H. Dihydroartemisinin induces apoptosis and
sensitizes human ovarian cancer cells to carboplatin therapy. J Cell Mol Med 2009;13(7):1358–70.
[98] Li PC, Lam E, Roos WP, Zdzienicka MZ, Kaina B, Efferth T. Artesunate derived
from traditional Chinese medicine induces DNA damage and repair. Cancer Res 2008;68(11):4347–51.
[99] Hou J, Wang D, Zhang R, Wang H. Experimental therapy of hepatoma with
artemisinin and its derivatives: in vitro and in vivo activity, chemosensitization, and mechanisms of action. Clin Cancer Res 2008;14(17):5519–30.
[100] Berdelle N, Nikolova T, Quiros S, Efferth T, Kaina B. Artesunate induces oxidative DNA damage, sustained DNA double-strand breaks, and the ATM/ ATR damage response in cancer cells. Mol Cancer Ther 2011;10(12):2224–33. [101] Huang C, Ba Q, Yue Q, Li J, Li J, Chu R, et al. Artemisinin rewires the protein interaction network in cancer cells: network analysis, pathway identification, and target prediction. Mol Biosyst 2013;9(12):3091–100.
[102] Li X, Ba Q, Liu Y, Yue Q, Chen P, Li J, et al. Dihydroartemisinin selectively inhibits PDGFR a-positive ovarian cancer growth and metastasis through inducing degradation of PDGFR α protein. Cell Discov 2017;3:17042.
[103] Efferth T, Benakis A, Romero MR, Tomicic M, Rauh R, Steinbach D, et al.
Enhancement of cytotoxicity of artemisinins toward cancer cells by ferrous iron. Free Radic Biol Med 2004;37(7):998–1009.
[104] Ba Q, Zhou N, Duan J, Chen T, Hao M, Yang X, et al. Dihydroartemisinin exerts its anticancer activity through depleting cellular iron via transferrin receptor-
1. PLoS One 2012;7(8):e42703.
[105] Zhang S, Gerhard GS. Heme mediates cytotoxicity from artemisinin and serves as a general anti-proliferation target. PLoS One 2009;4(10):e7472. [106] Stockwin LH, Han B, Yu SX, Hollingshead MG, ElSohly MA, Gul W, et al.
Artemisinin dimer anticancer activity correlates with heme-catalyzed reactive oxygen species generation and endoplasmic reticulum stress induction. Int J Cancer 2009;125(6):1266–75.
[107] Zhang S, Chen H, Gerhard GS. Heme synthesis increases artemisinin-induced radical formation and cytotoxicity that can be suppressed by superoxide scavengers. Chem Biol Interact 2010;186(1):30–5.
[108] Mercer AE, Copple IM, Maggs JL, O’Neill PM, Park BK. The role of heme and the mitochondrion in the chemical and molecular mechanisms of mammalian cell death induced by the artemisinin antimalarials. J Biol Chem 2011;286
(2):987–96.
[109] Hooda J, Cadinu D, Alam MM, Shah A, Cao TM, Sullivan LA, et al. Enhanced heme function and mitochondrial respiration promote the progression of lung cancer cells. PLoS One 2013;8(5):e63402. [110] Hooda J, Shah A, Zhang L. Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients 2014;6(3):1080–102.
[111] Hooda J, Alam M, Zhang L. Measurement of heme synthesis levels in mammalian cells. J Vis Exp 2015;101:e51579.
[112] Zhang X, Ba Q, Gu Z, Guo D, Zhou Y, Xu Y, et al. Fluorescent coumarinartemisinin
c o n j u ga te s a s m i to ch o n
d r i a-ta rget i n g t h
e ra n o st i c p ro b e s fo r
enhanced anticancer activities. Chemistry 2015;21(48):17415–21.
[113] Zhang CJ, Wang J, Zhang J, Lee YM, Feng G, Lim TK, et al. Mechanism-guided design and synthesis of a mitochondria-targeting artemisinin analogue with enhanced anticancer activity. Angew Chem Int Ed 2016;55(44):13770–4.
[114] Wang J, Zhang J, Shi Y, Xu C, Zhang C, Wong YK, et al. Mechanistic investigation of the specific anticancer property of artemisinin and its combination with aminolevulinic acid for enhanced anticolorectal cancer activity. ACS Cent Sci 2017;3(7):743–50.
[115] Wong YK, Xu C, Kalesh KA, He Y, Lin Q, Wong WSF, et al. Artemisinin as an anticancer drug: recent advances in target profiling and mechanisms of action. Med Res Rev 2017;37(6):1492–517.
[116] Dixon SJ, Lemberg KM, Lamprecht MR, Skouta R, Zaitsev EM, Gleason CE, et al.
Ferroptosis: an iron-dependent form of nonapoptotic cell death. Cell 2012;149(5):1060–72.
[117] Eling N, Reuter L, Hazin J, Hamacher-Brady A, Brady NR. Identification of artesunate as a specific activator of ferroptosis in pancreatic cancer cells.
Oncoscience 2015;2(5):517–32.
[118] Ooko E, Saeed ME, Kadioglu O, Sarvi S, Colak M, Elmasaoudi K, et al.
Artemisinin derivatives induce iron-dependent cell death (ferroptosis) in tumor cells. Phytomedicine 2015;22(11):1045–54.
[119] Yang ND, Tan SH, Ng S, Shi Y, Zhou J, Tan KS, et al. Artesunate induces cell death in human cancer cells via enhancing lysosomal function and lysosomal degradation of ferritin. J Biol Chem 2014;289(48):33425–41.
[120] Efferth T. From ancient herb to modern drug: Artemisia annua and artemisinin for cancer therapy. Semin Cancer Biol 2017;46:65–83.
[121] Abba ML, Patil N, Leupold JH, Saeed MEM, Efferth T, Allgayer H. Prevention of carcinogenesis and metastasis by artemisinin-type drugs. Cancer Lett 2018;429:11–8.
[122] Noori S, Hassan ZM. Dihydroartemisinin shift the immune response towards Th1, inhibit the tumor growth in vitro and in vivo. Cell Immunol 2011;271
(1):67–72.
[123] Farsam V, Hassan ZM, Zavaran-Hosseini A, Noori S, Mahdavi M, Ranjbar M.
Antitumor and immunomodulatory properties of artemether and its ability to reduce CD4+CD25+FoxP3+ T reg cells in vivo. Int Immunopharmacol 2011;11(11):1802–8.
[124] Zhang LX, Liu ZN, Ye J, Sha M, Qian H, Bu XH, et al. Artesunate exerts an antiimmunosuppressive effect on cervical cancer by inhibiting PG E2 production and Foxp3 expression. Cell Biol Int 2014;38(5):639–46.
[125] Cui C, Feng H, Shi X, Wang Y, Feng Z, Liu J, et al. Artesunate down-regulates immunosuppression from colorectal cancer Colon26 and RKO cells in vitro by decreasing transforming growth factor β1 and interleukin-10. Int Immunopharmacol 2015;27(1):110–21.
[126] Reiter C, Fr?hlich T, Gruber L, Hutterer C, Marschall M, Voigtl?nder C, et al.
Highly potent artemisinin-derived dimers and trimers: synthesis and evaluation of their antimalarial, antileukemia and antiviral activities.
Bioorg Med Chem 2015;23(17):5452–8.
[127] Fr?hlich T, ?apc? Karag?z A, Reiter C, Tsogoeva SB. Artemisinin-derived dimers: potent antimalarial and anticancer agents. J Med Chem 2016;59
(16):7360–88.
[128] Fr?hlich T, Ndreshkjana B, Muenzner JK, Reiter C, Hofmeister E, Mederer S, et al. Synthesis of novel hybrids of thymoquinone and artemisinin with high activity and selectivity against colon cancer. ChemMedChem 2017;12
(3):226–34.
[129] Efferth T. Cancer combination therapies with artemisinin-type drugs.
Biochem Pharmacol 2017;139:56–70.
[130] Fr?hlich T, Hahn F, Belmudes L, Leidenberger M, Friedrich O, Kappes B, et al.
Synthesis of artemisinin-derived dimers, trimers and dendrimers: investigation of their antimalarial and antiviral activities including putative mechanisms of action. Chemistry 2018;24(32):8103–13.
[131] Horwedel C, Tsogoeva SB, Wei S, Efferth T. Cytotoxicity of artesunic acid homo- and heterodimer molecules toward sensitive and multidrug-resistant CCRF-CEM leukemia cells. J Med Chem 2010;53(13):4842–8.
[132] Reiter C, Herrmann A, ?apci A, Efferth T, Tsogoeva SB. New artesunic acid homodimers: potent reversal agents of multidrug resistance in leukemia cells. Bioorg Med Chem 2012;20(18):5637–41.
[133] Reiter C, Capc? Karag?z A, Fr?hlich T, Klein V, Zeino M, Viertel K, et al.
Synthesis and study of cytotoxic activity of 1,2,4-trioxane- and egonolderived hybrid molecules against Plasmodium falciparum and multidrugresistant human leukemia cells. Eur J Med Chem 2014;75:403–12.
[134] Reiter C, Fr?hlich T, Zeino M, Marschall M, Bahsi H, Leidenberger M, et al.
New efficient artemisinin derived agents against human leukemia cells, human cytomegalovirus and Plasmodium falciparum: 2nd generation 1,2,4- trioxane-ferrocene hybrids. Eur J Med Chem 2015;97:164–72.
[135] Leto I, Coronnello M, Righeschi C, Bergonzi MC, Mini E, Bilia AR. Enhanced efficacy of artemisinin loaded in transferrin-conjugated liposomes versus stealth liposomes against HCT-8 colon cancer cells. ChemMedChem 2016;11
(16):1745–51.
[136] Bunnag D, Viravan C, Looareesuwan S, Karbwang J, Harinasuta T. Clinical trial
43 Author name et al. / Engineering 2(2016) xxx–xxx
of artesunate and artemether on multidrug resistant falciparum malaria in Thailand. A preliminary report. Southeast Asian J Trop Med Public Health 1991;22(3):380–5.
[137] Efferth T, Romero MR, Wolf DG, Stamminger T, Marin JJ, Marschall M. The antiviral activities of artemisinin and artesunate. Clin Infect Dis 2008;47
(6):804–11.
[138] Keiser J, Utzinger J. Artemisinins and synthetic trioxolanes in the treatment of helminth infections. Curr Opin Infect Dis 2007;20(6):605–12.
[139] Saeed MEM, Krishna S, Greten HJ, Kremsner PG, Efferth T. Antischistosomal activity of artemisinin derivatives in vivo and in patients. Pharmacol Res 2016;110:216–26.
[140] LamNS, Long X, SuXZ, LuF.Artemisinin and its derivatives intreatinghelminthic infections beyond schistosomiasis. Pharmacol Res 2018;133:77–100.
[141] Efferth T. Beyond malaria: the inhibition of viruses by artemisinin-type
compounds. Biotechnol Adv 2018;36(6):1730–7.
[142] Li J, Casteels T, Frogne T, Ingvorsen C, Honoré C, Courtney M, et al.
Artemisinins target GABAA receptor signaling and impair α cell identity.
Cell 2017;168(1–2):86–100.e15.
[143] Van der Meulen T, Lee S, Noordeloos E, Donaldson CJ, Adams MW, Noguchi GM, et al. Artemether does not turn α cells into β cells. Cell Metab 2018;27
(1). 218 25.e4.
[144] Ho WE, Cheng C, Peh HY, Xu F, Tannenbaum SR, Ong CN, et al. Anti-malarial drug artesunate ameliorates oxidative lung damage in experimental allergic asthma. Free Radic Biol Med 2012;53(3):498–507.
[145] Isacchi B, Arrigucci S, la Marca G, Bergonzi MC, Vannucchi MG, Novelli A, et al.
Conventional and long-circulating liposomes of artemisinin: preparation, characterization, and pharmacokinetic profile in mice. J Liposome Res 2011;21(3):237–44.
·新药发现与研究实例简析· 新药创制是复杂的智力活动, 涉及科学研究、技术创造、产品开发和医疗效果等多维科技活动。每个药物都有自身的研发轨迹, 而构建化学结构是最重要的环节, 因为它涵盖了药效、药代、安全性和生物药剂学等性质。 本栏目以药物化学视角, 对有代表性的药物的成功构建, 加以剖析和解读。 40多年前我国发现了青蒿素, 继之发明了青蒿琥酯、蒿甲醚和二氢青蒿素等药物, 对全球范围的疟疾治疗, 是一个划时代的变革与贡献, 挽救了数以百万计患者的生命与健康。在特殊的历史时期以举国体制研制新药, 决定了研发模式难以复制。研究者在大海捞针式的筛选试验中, 屠呦呦等从传统医药典籍中受到启发, 首先发现分离出青蒿素并确定了它的抗疟活性, 功不可没, 开创了青蒿素药物治疗的新领域, 因而她获得2015年诺贝尔医学或生理学奖, 当之无愧。接续的研究与开发, 在结构确证、化学合成、结构优化、工艺研究和临床研究等各个环节, 我国科学家同样做出了卓越贡献, 成就了由青蒿素演化成临床新药—青蒿琥酯、二氢青蒿素和蒿甲醚, 并在全球范围应用, 在抗疟药物中占据着中心地位。本文拟从化学和药物化学视角, 阐述从青蒿到发现青蒿素, 从青蒿素的发现到发明蒿甲醚和青蒿琥酯等药物的简要历程。(编者按) DOI: 10.16438/j.0513-4870.2015-1036 青蒿素类抗疟药的研制 郭宗儒 (中国医学科学院药物研究所, 北京 100050) 1青蒿素的研究背景 1.1 举国体制研究抗疟药物 20世纪60年代美国发动侵略越南战争, 当地疟疾肆虐, 疟原虫对已有药物产生耐药, 使战斗力严重减弱。应越南要求中国提供有效抗疟药物, 我国政府决定全国范围研究新型抗疟药, 遂于1967年5月23日成立了研究协作组, 简称“523任务”, 涵盖60多个研究单位, 500多位研究人员。在由启动研究到临床实验和应用的整个研发过程, 统一由“523任务”调度, 并非固定在一个研究单位中(张文虎. 创新中的社会关系: 围绕青蒿素的几个争论. 自然辩证法通讯. 2009, 31: 32?39)。 1.2从中药和民间药寻找药物或先导物 在“523任务”的诸多研究项目中, 有一个课题是“民间防治疟疾有效药物疗法的重点调查研究”, 这个研究小组获得了许多苗头, 例如从植物鹰爪分离出有效抗疟单体鹰爪甲素, 从陵水暗罗中分离出暗罗素的金属化合物,对常山乙碱的结构改造,以及青蒿素等。 1.3 青蒿和青蒿素的发现 1969年中国中医研究院中药研究所加入“中医中药专业组”。组长屠呦呦和组员余亚纲等从中医药古籍中搜集并筛选中草药单、复方数百种中, 余亚刚和顾国明发现青蒿呈现高频率(唐宋元明的医籍、本草和民间都曾提到有治疟作用)。通过广泛实验筛选, 聚焦到青蒿的乙醇提取物, 对疟原虫抑制率达到60%~80%, 虽然活性重复性差, 但为后来研究提供了有价值的参考(李国桥等. 青蒿素类抗疟药. 北京: 科学出版社, 2015: 3)。 屠呦呦从东晋葛洪《肘后备急方》阐述青蒿的用法得到了启发, “青蒿一握, 以水二升渍, 绞取汁, 尽服之”, 冷榨服用“绞汁”, 悟出可能不宜高温加热的道理, 并考虑到有效成分可能在亲脂部分, 遂改用乙醚提取, 于1971年10月在去除了酸性成分的中性提取物中, 分离得到的白色固体对鼠疟原虫的抑制率达100%。由绞汁联想低温提取, 但由水浸的冷榨液(通常含有水溶性成分) 怎样推论是脂溶性成分, 文献中无从考证。不过选择乙醚为萃取剂, 无疑是发现青蒿素、开辟青蒿素类药物治疗的关键一步。 用乙醚从黄花蒿分离出的倍半萜化合物除青蒿素(1, artemisinin) 外, 还鉴定了其他成分, 有青蒿
青蒿素体内药物代谢研究进展 廖文 (成都中医药大学成都 611137) 摘要:青蒿素是从植物青蒿中提取的一种具有抗疟作用的活性成分。近些年研究发现青蒿素不仅可以抗寄生虫,包括疟原虫、血吸虫,而且具有显著的抗炎、调节免疫和抗肿瘤等多方面的作用。本文主要介绍青蒿素抗疟作用的代谢机制,并对青蒿素的其他作用以及发展前景进行简要论述。 关键词:青蒿素;抗疟;代谢;其他作用;前景 Artemisinin in vivo drug metabolism research LIAO Wen (Chengdu University of Traditional Chinese Medicine, Chengdu 611137) Abstract:Artemisinin is extracted from the plant Artemisia annua with a role of the active ingredient anti-malarial. artemisinin recent study found that not only anti-parasites, including Plasmodium, Schistosoma, and has significant anti-inflammatory, immune regulation and anti-tumor effect, and many other. This paper describes the role of artemisinin-based antimalarial mechanisms of metabolism and the role of artemisinin as well as other future development brief. K ey words:artemisinin; malaria; metabolism; other role; prospects 青蒿素(artemisinin,QHS,结构式见图1)是我国 科研工作者于1972年首次从中草药青蒿中分离得到的 含过氧桥的新型倍半萜内酯。青蒿素结构独特、高效低 毒,具有清热解毒,抗肿瘤、抗菌、抗疟,增强免疫等 药理作用,对脑型疟、恶性疟等有特效,是我国唯一获 得国际认可的抗疟新药,已成为世界卫生组织推荐的治 疗疟疾的理想药物。我国青蒿资源十分丰富,目前其主 要产业资源也在我国。 (一)青蒿素的抗疟代谢作用 青蒿素类抗疟药临床应用以联合用药为主.从青蒿素的药理作用来看,它首先是被用于治疗疟疾,而且效果比以往的药物要好,因此主要用于该疾病的治疗。
青蒿主要药用成分青蒿素的衍生物是目前疗效最好 抗药性最低 Newly compiled on November 23, 2020
广西青蒿(黄花蒿)产业发展规划 广西壮族自治区农业厅 二○○年五月
目录
青蒿主要药用成分青蒿素的衍生物是目前疗效最好、抗药性最低、应用前景最好的抗疟药物,而且青蒿素在深度开发方面也有很好的市场前景。广西是全国2个青蒿素产品主要产地之一,随着全球市场对青蒿素的需求量不断扩大,青蒿产业面临良好的发展机遇。抓住机遇,加大工作力度,把广西壮族自治区建设成为青蒿生产基地的意义非常重大。按照自治区主要领导同志提出的“把广西建设成为青蒿生产基地”指示,充分发挥广西壮族自治区优势和特色,把握机遇,加快发展,培植国民经济新的增长点,探索中草药现代化产业开发新途径,制订本规划。 一、青蒿产业的现状及发展前景 (一)WHO改变用药配方,青蒿素需求强劲 据世界卫生组织(WHO)统计报告,全世界每年急性疟疾患者达3亿人,每年死于该病的人数约200-300万,90%的死亡病人发生在非洲,其中5岁以下儿童超过90%。曾是抗疟疾特效药的奎宁,长期使用后会产生广泛抗药性。而青蒿素类药物经多方试验,证明其在抗氯喹原虫耐药株恶性疟等方面有特殊疗效,1990年在越南疟疾患区使用,治愈率达97%,受到患区当地政府和患者的普遍欢迎。 2001年12月中旬, WHO的一份公报指出“治疗疟疾的最大希望来自中国”,肯定青蒿类药物为治疗疟疾的“首选药物”。2004年2月,WHO确定将青蒿琥酯、蒿
甲醚等青蒿素类药物作为全球新一代抗疟药,同时针对青蒿类药物半衰期短,治疗期较长(7天),价格较高的问题,推荐治疗期较短(3天)、相对便宜的以青蒿类药物为基础的联合用药(简称ACTs疗法),逐步取代传统的治疗疟疾方案。目前全球已有40个国家选择了ACT作为官方治疗疟疾用药,其中有36个国家用其作为一线治疗药物,4个国家作为二线药物,其它还有14个以上国家最近正考虑改换成ACT药物。据WHO统计,2003年全球抗疟药销售额约15亿美元,青蒿类药物销售额约为其1%,青蒿类药物市场空间巨大,发展前景看好。 2004年11月16日,由联合国儿童基金会、WHO、全球基金在哥本哈根召开了“全球抗疟药供应商预认证”会议。在这次会议上正式公布了联合用药的推荐处方及会议主持者的采购量,WHO对2004年的联合用药(ACTs)政策做了调整:确定了4个处方作为替代奎宁类的抗疟推荐用药,进入公共采购目录的药物主要包括青蒿琥酯和蒿甲醚等,以青蒿琥酯为主的联合用药2005年国际组织、机构的部分采购金额(不包括疟疾区各国政府的采购)共计4000万美元,2006年为4800万美元。估计各国政府采购金额、商业公司采购金额不会低于国际组织、机构的采购金额。目前青蒿素用药缺口为每年总需求的40~60%,估计填补全球青蒿(黄花蒿)种植的空缺需要15~20年。
青蒿素的合成与研究进展 摘要:青蒿素是目前世界上最有效的治疗疟疾的药物之一,存在活性好、毒副作用小、市场需求大、来源窄等特点。目前,青蒿素的获取途径主要有直接从青蒿中提取、化学合成和生物合成。本综述将针对近年来青蒿素的发展特点及合成方法进行论述。 关键词:青蒿素;合成方法;研究进展 青蒿素是中国学者在20世纪70年代初从中药黄花蒿( Artem isia annua L1 )中分离得到的抗疟有效单体化合物,是目前世界上最有效的治疗脑型疟疾和抗氯喹恶性疟疾的药物, 对恶性疟、间日疟都有效, 可用于凶险型疟疾的抢救和抗氯喹病例的治疗。青蒿素还具有抑制淋巴细胞的增殖和细胞毒性的用1;具有影响人体白血病U937细胞的凋亡及分化的作用2;还具有部分逆转MCF-7/ARD细胞耐药性作用3;还具有抑制人胃癌裸鼠移植瘤的生长的作用4;还具有一定的抗肿瘤作用5等。除此之外,青蒿素及其衍生物还具有生物抗炎免疫作用、生物抗肿瘤作用、抑制神经母细胞瘤细胞增殖的作用等。世界卫生组织确定为治疗疟疾的首选药物, 具有快速、高效、和低毒副作用的特征。6。因在发现青蒿素过程中的杰出贡献,屠呦呦先后被授予2011年度拉斯克临床
医学研究奖和2015年诺贝尔医学奖。 1 青蒿素的理化性质及来源 青蒿素的分子式为C15H22O5, 相对分子质量为282. 33。是一种含有过氧桥结构的新型倍半萜内酯,有一个包括过氧化物在内的1,2,4-三烷结构单元,它的分子中还包括7个手性中心,合成难度很大。中国科学院有机所经过研究,解决了架设过氧桥难题,在1983年完成了青蒿素的全合成。青蒿素也有一些缺点, 如在水和油中的溶解度比较小, 不能制成针剂使用等。 2 青蒿中提取青蒿素 青蒿素是从菊科植物黄花蒿中提取出来的含有过氧桥的倍半萜内酯类化合物,在治疗疟疾方面具有起效快、疗效好、使用安全等特点。目前主要的提取方法有溶剂提取法、超临界提取法、超声波萃取法、微波萃取法、其他萃取法等。2.1有机溶剂萃取青蒿素 水蒸气蒸馏(steam distillation,SD)法由于其具有设备简单,操作安全,不污染环境,成本低,避免了提取过程中有机溶剂残留对油质造成影响等特点,是有效提取中药挥发油的重要方法。有机溶剂提取法是目前青蒿中许多有效成分的提取目前仍然常用的方法,常用的溶剂有醇类(甲醇、乙醇
青蒿素类抗疟药的研究进展 【摘要】青蒿素及其衍生物是一类全新结构的抗疟药,具有抗疟作用迅速、高效、低毒,且与大多数抗疟药无交叉抗性等特点。 【关键词】:青蒿素;抗疟;作用机制。 Abstract:Artemisinin and its derivatives with endoperoxide function are new and important antimalarial drugs,and their antimalarial action is quick,efficient and without cross resistance. key words:artemisinins;antimalarial;action mechanism. 疟疾是目前最严重的传染病之一,每年有大约5亿人患疟疾,死亡人口数达275万之多【1】。在众多的抗疟药物中,青篙素类药物独树一帜。青篙素及其衍生物的抗疟作用是我国科技工作者从中国的传统中草药中发现的。它们具有独特的化学结构和作用机制,抗疟效果非常明显,作用快,毒性低,而且价格便宜,因此颇受全球医药工作者和广大疟疾患者的青睐。从七十年代始,国内外己有卜千篇青篙素及其衍生物的有关研究报道,本文拟就青篙素类药物抗疟作用机制的近年研究进展作一综述。 一、细胞水平的研究 1.青篙素类药物与血细胞结合 青篙素及其衍生物通过与尚未确定的受体结合而选择性地集中在被疟原虫感染的红细胞,被感染的红细胞中的青篙素浓度是末被感染红细胞中的青篙素浓度的100多倍【2】。Asawamahasakda和他的同事们【3】发现用3H标记的青篙素被分离的红细胞膜吸收,但却不能被末感染的红细胞吸收。超过一半的膜关联药物能被乙酸乙醋抽提的磷脂酶A:所分解.41-42%的残留药物似乎与红细胞膜蛋白结合。 2.引起疟原虫细胞超微结构变化 青篙素及其衍生物能较其它抗疟疾药物更具抗疟效果,必定有其独特的作用机制。为探明其作用机制,科学家们进行了大量直有成效的工作。早期通过光学显微镜技术、电子显微镜技术等,观察到青篙素类药物主要作用于疟原虫的膜结构。在红细胞内期,青篙素及其衍生物能引起疟原虫膜结构发生变化,如由胞膜部分形成食物泡、核质,线粒体、内质网、核膜等也相应地出现相关变化,这些变化最终导致自噬泡形成并使细胞质减少,从而致死疟原虫【4】。 3.影响营养物质运输 红细咆内期原,虫被纳虫泡包.裹,许多管状饱从泡膜上突出出来、形成复杂的网络,伸向红细胞周边,是疟原虫获得外源性营养物质的通道,同时可运输包括青篙素类小分子药物通过,因此管状泡网被认为是感染疟原虫红细胞内能聚集大量青蒿素类药物的前提【5】。有人研究发现,青篙素类药物可破坏管状泡网的组成及膜结构,从而破坏其转运营养物质功能力。 二、生物化学及分子水平的研究 1.过氧桥与抗疟作用
【摘要】为了解青蒿素类药物的药理和毒理学研究进展,笔者查阅有关文献 ,综述了青蒿素类药物的药理与毒理学研究进展。研究结果表明:药动学研究显示此类药物吸收快、分布广、代谢与排泄快;青蒿素类药物除具有抗疟作用外,还有免疫调节、抗肿瘤、抗炎、抗血吸虫及其它寄生虫等作用;无严重的不良反应。 【关键词】青蒿素;药效学;药动学;毒理学 青蒿素是我国药学工作者于1971年从植物黄花蒿atemisia annua l.叶中提取分离得到的一个具有过氧桥的倍半萜内酯,经化学改造可生成多种衍生物,如蒿甲醚、双氢蒿甲醚、青蒿酯钠、青蒿琥酯等均具有高效低毒的抗疟活性,尤其对具有抗氯喹能力的脑疟和急性疟有效,同时,对青蒿素类药物的研究引起了全世界药学工作者的关注,发现了青蒿素类药物许多新的药理活性和一些毒理作用,作者就近年来青蒿素类药物的药理和毒理学方面的研究进展作一综述。 1 青蒿素的药理学研究 1.1 药代动力学中国青蒿素研究小组经大鼠实验证明[1],大鼠口服青蒿素150mg/kg后,吸收迅速完全,但血药浓度低,维持时间短,显示有首过效应。静脉注射青蒿素混悬水溶液150mg/kg血药时程符合二室模型,t1/2为30min,vd为4.1l/kg,表明青蒿素在体内分布广泛,消除迅速。在人体肌内注射蒿甲醚油剂3.2mg/kg,6.0mg/kg,和10.0mg/kg后,血药浓度达峰时间为4h~6h,平均潴留时间分别为10.2h、15.6h和19.0h,显示经肌内注射后蒿甲醚可在体内存留较长时间[2],在人体静脉注射青蒿琥酯钠 2.0mg/kg和 3.8mg/kg后,血药时程符合二室模型,t1/2分别为30min和36min~48min.给药后7h内尿中累积排出原型药物仅占给药量的0.1%~6.8%,说明该药在体内的消除方式主要是代谢转化。文献报道[2]青蒿琥酯进入体内后很快就转化成二氢青蒿素。用家免法测定体液中的药物浓度,难以对二氢青蒿素和青蒿琥酯作出区别,所测的浓度很可能是二种物质浓度的总和。 1.2 青蒿素类药物的药效学研究 1.2.1 抗肿瘤作用文献报道[3]青蒿酯钠在体外对小鼠p388细胞、hela细胞、人肝癌smmc-7721细胞、人鼻咽低分化鳞癌cne2、sune-1及体内抑瘤实验对肝癌、网状红细胞肉瘤及裸鼠移植人鼻咽癌等有肿瘤抑制作用。青蒿琥酯对宫颈癌细胞系hela细胞抑制的半抑菌浓度(ic50)在37μg/ml左右,提示青蒿素衍生物有选择性杀伤癌细胞的作用。青蒿琥酯具有放射增敏作用与 miso相比较,10μg/ml青蒿琥酯增敏作用与miso相当,而30μg/ml的青蒿琥酯增敏效果大于miso。氧效应可增加肿瘤细胞对光照的敏感性,放射增敏剂可以增强射线对肿瘤的杀伤能力,尤其有助于解决实体肿瘤中缺乏氧细胞对射线的抗放射性而导致的肿瘤放疗治愈率低的难题,鉴于青蒿琥酯分子中含有过氧桥结构,在与癌细胞接触时可能使氧释放发生了模拟氧作用,从而增加hela细胞对放射敏感性的作用[4]。青蒿琥酯是否能成为新一代的放射增敏剂以及进一步的作用机理尚待深入研究[6]。 1.2.2 抗孕作用文献报道[5~7]二氢青蒿素与青蒿琥酯对金黄地鼠与豚鼠胚胎的影响和同类药物对大、小鼠胚胎的影响,既有区别又有相似。其主要区别是在大鼠和小鼠身上药物的作用以引起胚胎的吸收为主,而在豚鼠身上药物的作用则以引起流产为主。其相似点是当药物剂量偏小时侥幸存活下来的胎儿仍能正常生长,基本未见畸形。二氢青蒿素单次sc给药终止早孕的ed50为6.1mg/kg,而成年雌性地鼠的近似致死量为170mg/kg,,后者为前者的28倍。青蒿琥酯钠分多次sc给药,抗早孕的ed50为4.0mg/kg(4次总量)而对成年雌性地鼠的近似致死量为135mg/kg,后者是前者的34倍。流产后的地鼠可于7~10d内接受交配并怀孕。故该俩药对胚胎的毒性要比母体大得多。又从给药动物的子宫和卵巢的切片上可看到给药后动物宫腔内有坏死的胚胎组织,胚体的坏死较胎盘为早而子宫内膜及肌层未见明显损伤,卵巢中的卵泡完全正常。此项结果表明,二氢青蒿素与青蒿琥酯对胚胎有相当高的选择性毒性,较低剂量即可致胚胎死亡而引起流产,对母体子宫及卵巢影响却不明显。因此,二
科教论坛农村经济与科技2019年第30卷第12期(总第464期) 青蒿(Artemisia?carvifolia),别名草蒿,属菊科类一年生或二年生草本植物,青蒿素(Artemisinin)是20世纪70年代我国药学人员从菊科植物黄花蒿叶中提取的含过氧化基团结构的倍半萜内酯化合物。青蒿素的主要衍生物包括蒿甲醚(Artemethere)、蒿乙醚(Arteether)、青蒿琥酯(Artesunate)、二氢青蒿素(Dihydro?artemisinin)等。以往的报道中,青蒿素类药物主要以治疗疟疾为主,随着研究的不断深入,发现青蒿素类化合物还有许多的作用,如抗炎、抗孕、治疗艾滋病和肿瘤等。目前,临床上青蒿素类药物大量存在溶解度差、生物利用度低、首过效应高、疟原虫复燃率高、给药频繁等问题,因此,近年来青蒿素类药物的剂型研究便成为了热点。 随着制药科技的发展,很多新技术运用到青蒿素及其衍生物的制剂中来,为青蒿素多方面的治疗作用提供了可能的途径,其中,最受瞩目的为纳米制剂、固体分散体、包合物、微乳、经皮给药制剂。 1?纳米制剂 纳米给药系统为一系列粒径在纳米级的新型微小给药系统的统称,根据纳米颗粒分散运动状态及其性质的特殊性,纳米给药系统主要可以分为:纳米粒、脂质体、纳米乳、聚合物胶束、纳米混悬剂等。该系统具有良好的肿瘤靶向性,较长的体内循环时间,易被细胞摄取,可控制药物释放以及改善药物溶解度,增加药物稳定性等特点。 1.1?纳米乳 纳米乳(nano?emulsion)是由表面活性剂、助表面活性剂、油相、水相组成的一种稳定透明的胶体分散系统,?其粒径在10?~?100?nm之间。胡宏伟、刘根新等在研究用青蒿琥酯治疗牛、羊泰勒焦虫病及双芽焦虫病时,乳化剂选择聚山梨醇酯-80,助表面活性剂选择正丁醇,油酸乙酯为油相制备青蒿琥酯纳米乳注射剂。解决了青蒿琥酯在水中的溶解度不大,?口服不能避免肝脏的首过效应,?市售青蒿琥酯钠盐放置不稳定,?临床使用不方便的问题。 1.2?纳米粒 纳米粒(nanopartilcles,NP)由天然或合成高分子材料制成,是一种粒径介于1~100nm固态胶体粒子,包括纳米球(Nanospheres)和纳米囊(Nanocapsules)。活性组分(药物、生物活性材料等)能溶解、包裹于粒子内部,或者吸附、附着于粒子表面。?王霜用改良自乳化/溶剂扩散法将青蒿琥酯制成适用于人体可生物降解的纳米粒,并将肿瘤细胞表面特异性的可识别配体?Tf结合在载药纳米载体上,实现对肿瘤组织(细胞)的靶向治疗,?动物体内实验表明该新型纳米制剂具有血液及骨髓的靶向性。王东采用初生态微晶法制备了载有蒿甲醚的纳米胶囊,解决了蒿甲醚不溶于水、代谢快及利用率低的缺点,可显著提高药效。 1.3?纳米脂质体 纳米结构脂质载体(?nanostructured?lipid?carrier,?NLC)是以一定比例的液态油或其他不同的脂质(如卵磷脂、甘油三酯等)为载体,将药物包裹于类脂核中的固态胶体给药体系,粒径在50~1000?nm之间,?已被公认是一种新型的纳米给药系统。张晓云,赵鹏等采用动物肿瘤膜型研究双氢青蒿素纳米脂质载体与双氢青蒿素混悬液对肝癌瘤株的抑制作用,证实双氢青蒿素纳米脂质载体较普通混悬液对白血病细胞K562?及胶质瘤细胞U87?具有更强的增殖抑制作用,为开发高效低毒的双氢青蒿素抗癌药物提供依据。赵春霞,沈雪松等用青蒿琥酯纳米脂质体干预血管内皮生长因子(?VEGF)?及血管内皮细胞生长因子受体2(?VEGFR2)?在HepG2?中的表达,证明青蒿琥酯纳米脂质体能够抑制肿瘤血管的生成达到抗肿瘤作用,且作用强于青蒿琥酯原料药,有应用于肝癌治疗的潜在价值。 2?固体分散体 固体分散体是指药物高度分散在适宜的载体材料中类似于液体系统,形成的一种固态物质。固体分散体使得药物以无定型太、微晶态、分子分散态或胶体分散态存在,分散度很大,当与胃肠中液体接触后,溶出速度加快,药物的吸收加快,生物利用度提高。根据载体性质的不同和释药特点的不同,固体分散体又分为速释型固体分散体、缓控释型固体分散体和肠溶型固体分散体。 2.1?速释型固体分散体 速释型固体分散体是利用亲水性载体材料制备的固体分散体。药物在载体材料中高度分散,由于载体材料的亲水性,使 青蒿素类药物新剂型研究进展 李文婷1,2,张国丽2,张锐武2,段国蕾2,杨兆祥2 (1.楚雄医药高等专科学校,云南?楚雄?675005;? 2.昆药集团股份有限公司,云南?昆明?650106) [摘 要]青蒿素类的药物因为其抗疟疾的疗效为人熟知,随着研究的深入,青蒿素类化合物显现出多方面的临 床作用,近年来对肿瘤的治疗成为关注的热门,随之而来的剂型研究也成为了热点。随着制药科技的发展,新剂型与 新技术也运用到了青蒿素类药物的制剂过程中来,现查阅文献,对近年来国内外青蒿素类药物新剂型的研究进展进行 归纳总结。 [关键词]青蒿素;新剂型;抗肿瘤 [中图分类号]R284 [文献标识码]A [收稿日期]2019-04-01 -299-
青蒿素性质及合成方法 院系:化工学院 专业:应用化学 学号: : 指导老师: 2016/1/12
摘要:青蒿素是目前治疗疟疾的特效药。本文对自青蒿素发现以来的最新研究 进展进行了比较详尽的综述。容包括:青蒿素的特性,青蒿素的合成,青蒿素的生物合成,青蒿素衍生物。 关键词:青蒿素;合成方法;青蒿素衍生物 Abstract:The recent research advances in artemisinin, the most effective weapons against malarial parasites have been reviewed. An overview is given on artemisinin research from the following aspects:sources of artemisinin,synthesisof artemisinin, biosynthesis of artemisinin, analogs of artemisinin and artemisinin production from plant tissue cultures。 Key words:artemisinin,synthesis,artemisinin derivatives 目录
1、前言……………………………………………………………… 2、青蒿素的基本性质………………………………………………(1)分子结构…………………………………………………………(2)理化性质…………………………………………………………(3)药动力……………………………………………………………(4)提取工艺………………………………………………………… 3、合成方法…………………………………………………………(1)全合成…………………………………………………………(2)半合成…………………………………………………………(3)生物合成……………………………………………………… 4、衍生物………………………………………………………… 5、抗癌功能………………………………………………………… 6.结论………………………………………………………………
您的位置:在线学习->第十一章抗生素类药物分析(1) 第十一章抗生素类药物分析 基本要求 学习要点 内容 第一节概述 一、特点:化学纯度较低, 同系物多,异构体多,降解物多,稳定性差。 二、鉴别方法:生物学法,理化方法。 三、特殊检查项目:异常毒性、热源或细菌内毒素、降压物质、无菌,组分分析,聚合物等。 四、含量测定或效价测定 (一)、微生物学法——通过比较标准品与供试品产生抑菌圈的大小来测定供试品的效价。 其原理恰好与临床应用要求一致,更能确定抗生素的医疗价值。 1、对于分子结构复杂、多组分的抗生素,生物学法是首选的效价测定方法。 2、本法的优点: 灵敏、用量小,结果直观 适用范围广:纯度好的、差的制品,已知或新发现的抗生素均适用,同一类型的抗 生素不需分离,可一次测定其总效价。 3、缺点: 操作步骤多,测定时间长,误差大等。 (二)、理化方法——适用于提纯的产品以及化学结构已确定的抗生素。 1、本法的优点: 迅速、准确、有较高的专属性。 2、缺点: 对含有具同样官能团杂质的供试品不适用,或需采取适当方法加以校正。而且当该法是利用某一类型抗生素的共同结构部分的反应时,所测得的结果,往往只能代表药物的总的含量,并不一定能代表抗生素的生物效价。 第二节β-内酰胺类抗生素 一、化学结构与性质 (一)、青霉素族
(二)、头孢菌素族 二、鉴别试验 (一)、呈色反应 1、羟肟酸铁反应青霉素及头孢菌素在碱性中与羟胺作用,β-内酰胺环破裂生成羟肟酸;在稀酸中与高铁离子呈色。 2、茚三酮反应 3、与重氮苯磺酸的偶合反应 4、硫酸-甲醛试验 第1页/共8页 您的位置:在线学习->第十一章抗生素类药物分析(2) (二)、各种盐的反应 1、钾、钠离子的火焰反应 2、有机胺盐的特殊反应(如普鲁卡因青霉素的重氮化-偶合反应) (三)、色谱法 1、高效液相色谱法(HPLC) 2、薄层色谱法(TLC) 3、中国药典收载的头孢菌素族药物和大多数青霉素族药物采用HPLC法进行鉴别。 (四)、光谱法 1、IR——各国药典对收载的β-内酰胺类抗生素几乎均采用了本法进行鉴别。 2、该类抗生素共有的特征峰: 1)、β-内酰胺环羰基的伸缩振动(1750~1800) 2)、仲酰胺的氨基、羰基的伸缩振动(3300cm-1±,1525 cm-1±,1680 cm-1±) 3)、羧酸离子的伸缩振动(1600 cm-1±、1410 cm-1±) 3、UV——利用最大吸收波长鉴定法或利用水解产物的最大吸收波长鉴定法。 三、特殊杂质的检查 本类抗生素的特殊杂质主要有高分子聚合物,有关物质,异构体等,一般采用HPLC法控制其量,也有采用测定杂质的吸收度来控制杂质量的。 (一)、聚合物——HPLC法 1、色谱条件与系统适用性试验用葡聚糖凝胶G-10(40~120?m)为填充剂,玻璃柱内 径1.3~1.5cm,床体积50~60mL;流动相A为含3.5%硫酸铵的0.01mol/L磷酸盐缓冲液(取磷 酸氢二钠 2.19g和磷酸二氢钠0.54g,加水1000mL使溶解,调节pH值至7.0),流动相B为0.01%十二烷基硫酸钠溶液;流速为每分钟1mL;检测波长为254nm。以流动相A为流动相,用1mg/mL
中国科学: 生命科学 2012年 第42卷 第5期: 345 ~ 354 SCIENTIA SINICA Vitae https://www.doczj.com/doc/8513572562.html, https://www.doczj.com/doc/8513572562.html, 英文引用格式: Sun C, Li J, Zhou B. Mechanism of action of artemisinins: a long unsettled challenge. SCIENTIA SINICA Vitae, 2012, 42: 345–354, doi: 10.1360/052012-168 《中国科学》杂志社 SCIENCE CHINA PRESS 评 述 青蒿素类药物的作用机制: 一个长久未决的基础 研究挑战 孙辰, 李坚, 周兵* 清华大学生命科学学院, 生物膜与膜生物国家重点实验室, 北京 100084 * 联系人, E-mail: zhoubing@https://www.doczj.com/doc/8513572562.html, 收稿日期: 2012-04-20; 接受日期: 2012-04-24 doi: 10.1360/052012-168 摘要 青蒿素是中国自主研制的抗疟良药, 高效、低毒, 许多基于青蒿素研发的衍生物具有良好的抗疟效果, 近年来已成为抗疟的一线药物, 受到世界医疗卫生界的充分肯定. 虽然青蒿素结构奇特, 抑疟效果显著, 但40年来其生物作用机制之谜一直未被彻底破解. 针对青蒿素类药物的作用机制, 提出了不同的假说, 如血红素参与青蒿素的激活并被烷基化从而起到抑疟作用, 线粒体参与青蒿素的激活和作用过程, 某些特定的蛋白是青蒿素作用靶点等. 除抑疟外, 青蒿素类药物在杀灭其他种类寄生虫、抑制某些癌症细胞以及抗病毒、治疗类风湿等方面也有一定作用. 本文将对青蒿素类药物作用机制的研究进行综述及展望, 包括抗疟疾过程中的药物激活、作用靶点以及简要的青蒿素抑制肿瘤细胞作用机制, 以期为今后的研究提供帮助. 关键词 青蒿素 作用机制 血红素 线粒体 2011年9月, 中国中医科学院科学家屠呦呦获得美国拉斯克临床医学奖, 以表彰她在抗疟药物青蒿素(artemisinin)开发过程中的贡献. 一时间, 疟疾和抗疟良药青蒿素成为国人关注的焦点. 疟疾是严重影响人体健康的传染性疾病, 尤其在非洲、南亚、东南亚及南美洲大陆的热带亚热带地区发病严重. 世界卫生组织统计报告显示, 疟疾2010年发病人数为2.16亿, 造成约65.5万人死亡, 其中86%的受害者是5岁以下儿童[1]. 青蒿素的发现是中国20世纪70年代“中国疟疾防治药物研究工作协作项目”(又称“523”科研项目)中的一项重要成果, 中国科学家们的协作研发为世界人民抗击疟疾做出了重要贡献. 青蒿素对红内期疟 原虫有直接杀灭作用, 快速高效且毒性低, 缺点是半衰期比较短, 单独使用再燃率较高. 其他治疗疟疾的药物, 如氯喹、甲氟喹和奎宁等均出现了抗药株, 而青蒿素类药物自投入使用以来, 除在柬埔寨地区出现青蒿琥酯对疟原虫清除效率降低的病例(体外实验并没有出现类似的延缓现象)[2], 尚无确证的青蒿素类药物抗性疟原虫出现. 为防止将来青蒿素抗性菌株的出现, 世界卫生组织颁布了 “青蒿素联合疗法”(artemisinin combination therapy, ACT). 除治疗疟疾的良好效果外, 青蒿素在杀灭其他种类寄生虫, 抑制某些癌症细胞以及抗病毒、治疗类风湿等方面也有一定作用. 青蒿素的治疗效果举世瞩目, 但其作用机制至今仍是一个谜, 也是一个长期
第十五章抗生素类药物的分析 一、选择题 【a型题】 1.《中国药典》规定检查青霉素钠中水分的原因在于() A.水分是活性物质 B.水分易使青霉素发霉 C.水分影响青霉素钠的质量 D.水分影响青霉素钠的含量测定结果 E.青霉素钠遇水可水解而失效 2. 规定检查c组分的药物是( ) A.青霉素钾 B.头孢羟氨苄 C.罗红霉素 D.硫酸庆大霉素 E.盐酸四环素 3.《中国药典》采用HPLC加校正因子的主成份对照法进行杂质检查的是( ) A.青霉素钠 B.盐酸四环素 C.阿莫西林 D.罗红霉素 E.头孢羟氨苄 方法是( ) 4.《中国药典》测定维生素B 1 A.紫外分光光度法 B.碘量法 C.铈量法 D.非水滴定法 E.溴酸钾滴定法 5.《中国药典》检查青霉素中聚合物的方法( ) A.对照品比较法 B.凝胶色谱法 C.高效液相 D.气相色谱 E.紫外分光光度法 6. 下列反应属于链霉素特征鉴别反应的是() A.茚三酮反应 B.麦芽酚反应 C.有N-甲基葡萄糖胺反应 D.硫酸-硝酸呈色反应 7. 青霉素不具有下列哪类性质() A.含有手性碳,具有旋光性 B.分子中的环状部分无紫外吸收,但其侧链部分有紫外吸收 C.遇硫酸-甲醛试剂有呈色反应可供鉴别 D.具有碱性,可与无机酸形成盐
8. 碘与青霉噻唑酸的反应是在() A.强酸性中进行 B.在强碱性中进行 D.中性中进行 9. 青霉素在碱或青霉素酶作用下的水解产物是() A.青霉烯酸 B.青霉酸 C.青霉胺 D.青霉醛 10. 抗生素的常规检查项目不包括() A.鉴别试验 B.异常毒性试验 C.热原试验 D.水分测定 E.升压试验 11. 碘量法测定维生素C注射液含量时,需用试剂不包括() A.丙酮 B.甲醛 C.淀粉指示液 D.稀醋酸 E.碘滴定液 12. 下列化学性质中不正确的是() A.青霉素族药物具有紫外吸收 B.链霉素在碱性条件下较稳定 C.四环素具有酸碱两性 D.氯霉素在无水乙醇中显右旋 E.红霉素在pH>8时发生水解 【b型题】 A.青霉素钾 B.头孢羟氨苄 C.罗红霉素 D.硫酸庆大霉素 E.盐酸四环素 1. 茚三酮反应( ) 2. 三氯化铁反应( )
青蒿素的发现,提取及一系列发展应用 1.时代背景:时代背景.mp4 世界上影响人数最多的疾病并非现在深受关注的艾滋病,而是一种堪称“历史悠久”的疾病——疟疾,也就是俗称的“打摆子”,同时,它也是当今除艾滋病外,上升趋势最为显著的一种传染病,每年2~3亿人感染此病,200多万人死亡。19世纪从南美洲金鸡纳树皮中得到的奎宁曾成为最有效的药物,治愈了众多的疟疾患者。20世纪第二次世界大战后模仿奎宁基本结构而合成的一批新药如氯喹、伯喹也曾救治过无数的病人。但是20世纪60年代出现抗药性疟原虫后,以往常用的抗疟药(如氯喹、磺胺、奎宁等)的效果便不复存在,以至于造成了无药可医的局面,特别在东南亚、非洲地区情况更为严重。青蒿素类药物的出现以其副作用低且不易产生抗药性而被誉为“治疗疟疾的最大希望”。 2. 什么是青蒿素时代背景.mp4 ◆分子式为C15H22O5,分子量282.33,组分含量:C 63.81%,H 7.85%,O 28.33%。 ◆无色针状晶体,味苦。 ◆在丙酮、醋酸乙酯、氯仿、苯及冰醋酸中易溶,在乙醇和甲醇、乙醚及石油醚中可溶解,在水中几乎不溶。
青蒿素(Artemisinin)又名黄蒿素,是一种具有过氧桥的倍半萜内酯类化合物。分子式为C15H22O5,分子量为282.34,具有过氧键和δ-内酯环,有一个包括氧化物在内的1,2,4-三恶烷结构单元,在自然界中是非常罕见的,它的分子中包括7个手性中心。青蒿素为无色针状结晶,熔点为156~157℃,易溶于氯仿、丙酮、乙酸乙酯和苯,
可溶于乙醇、乙醚,微溶于冷石油醚,几乎不溶于水。因其具有特殊的过氧基团,对热不稳易受湿、热和还原性物质的影响而分解。 3.为什么要选用青蒿治疗疟疾? 疟疾是一个非常古老的疾病。我们的先人对它还是有一定办法的。在晋代葛洪所著的《肘后备急方》中就有关于疟疾的治疗方药,原文如下:青蒿一握,以水二升渍,绞取汁,尽服之。意思是,用一把青蒿,以二升的水浸渍以后,绞扭青蒿,取得药汁,然后一次服尽。可别小看这几句话,它说明,我们的古人对于青蒿截疟已经有了很深入的认识。 4.验证青蒿素对疟疾的治疗效果实验: 为什么在实验室里青蒿的提取物不能很有效地抑制疟疾呢?是提取方法有问题?还是做实验的老鼠有问题? “青蒿一握,以水二升渍,绞取汁,尽服之”为什么这和中药常用的高温煎熬法不同?原来古人用的是青蒿鲜汁!温度!这两者的差别是温度!很有可能在高温的情况下,青蒿的有效成分就被破坏掉了。改用沸点较低的乙醚进行实验,她在60摄氏度下制取青蒿提取物。接下来在实验室里,青蒿提取物对疟原虫的抑制率达到了100%!
青蒿素类抗疟药研究进展 谭佳佳2009072114 药剂一班 摘要:本文叙述了疟疾的危害性,详细介绍了青蒿素的抗疟疾机制,青蒿素的联合用药,以及青蒿素的复方制剂及其出现的抗药性。 关键词:青蒿素抗疟疾抗药性 疟疾在夏秋季流行。在热带亚热带地区,一年四季都可发病。经疟蚊叮咬或输入带疟原虫者的血液而感染。疾病的病原体是疟原虫(plasmodium,spp)。疟原虫有130余种,主要寄生于人和哺乳动物,少数寄生在鸟类和爬行类动物。疟原虫有严格的宿主选择性。侵袭人类的疟原虫有4种:间日疟原虫(plasmodi—um vivax)、三日疟原虫(plasmodium malariae)、恶性疟原虫(plas—modium falciparnm)和卵圆疟原虫(plasmodium ovale)。恶性疟原虫是东南亚和非洲流行疟疾的主要病原体,是造成患者死亡的主要杀手。疟原虫生活史可分为有性生殖和无性生殖两个阶段,前者在雌性按蚊体内进行,后者在人体内完成。人体内无性生殖又分原发性红细胞外期、继发性红细胞外期和红细胞内期(红内期)等阶段[1]。疟疾主要流行地区是在非洲中部、南亚、东南亚和南美NJk部地区,其中非洲的疫情最为严重[2]。在我国疟疾主要流行在华南华中的丛林多山地区,但疫情远较非洲为轻。儿童、孕妇、旅游者和新移民是易患疟疾的高危人群。恶性疟疾患者如果没有得到及时有效的治疗,病死率非常高。在热带亚热带地区,恶性疟疾是一种十分可怕的疾病。 全世界有40%左右的人口受到疟疾的威胁,目前治疗疟疾的一线药物首选青蒿素(世界卫生组织推荐)。黄花蒿(Artemisia annua L.)属菊科草本植物,俗名青蒿,在我国已经有2000余年的药用历史,是提取青蒿素的唯一原料药材。我国黄花蒿种质资源丰富,种植面积和青蒿素产量占全世界的90%以上。其中,重庆市是全国黄花蒿的优质产区,种植面积和青蒿素产量分别占全国的70%和80%,是当地的主要经济作物。据重庆市海关统计,2009年1至9月我国青蒿素成药出口634t,70%出口非洲,30%出口美洲、亚洲和欧洲,为人类防治疟疾做出了巨大贡献。[3]青蒿素是我国药学工作者在1971年从菊科植物黄花蒿叶中提取分离得到的一种具有过氧桥结构的倍半萜内酯类化合物,它是我国在世界上首次研制成功的一种抗疟新药。在青蒿素的基础上,经过结构改造,又得到蒿甲醚、蒿乙醚、青蒿琥酯等衍生物。青蒿素类药物以其能快速有效地杀灭各种红细胞内期疟原虫和低毒性而成为抗疟首选药。国内外有大量论文报导该类化合物的化学、药学、药理和临床研究结果。本文对青蒿素类药物抗疟机制、联合用药予以综述。 1 青蒿素抗疟机制 青蒿素及其衍生物被全世界公认为是一种很有效的抗疟新药,但其抗疟作用机制至今仍然不十分明确。青蒿素的作用机制在早期认为是对红细胞阶段的恶性疟原虫有直接杀死作用。但后来发现青蒿素及其衍生物的浓度比产生抗疟活性浓度高很多才显示细胞毒作用[4]。随着对青蒿素抗疟机制进一步研究,发现青蒿素类化合物抗疟作用属于氧化性机制,与疟原虫体内的铁有重要关系。当青蒿素被疟原虫体内的铁催化,其结构中的过氧基团环分裂产生有破坏生理作用的氧化性自由基[5]。氧化性自由基与疟原虫蛋白络合形成共价键,使疟原虫蛋白失去功能,从而导致虫体死亡。近年来,又有很多学者在基因水平上研究,认为青蒿素可能通过阻断疟原虫的PfA TP6酶活性而产生抗疟作用。PfA TP6酶原本通过将钙离子排出细胞,来调节人体钙平衡。当它停止工作时,细胞内钙水平升高,细胞随之凋亡,继而达到抗疟效果。Eckstein—Ludwig等[6]通过荧光实验证明青蒿素通过阻断疟原虫所在细胞PfA TP6
理化性质 青蒿素(Artemisinin)是从复合花序植物黄花蒿(Artemisia annua L.,即中药青蒿)中提取得到的一种无色针 昆明地区青篙素标准品红外光谱图 状晶体,化学名称为(3R,5aS,6R,8aS,9R,12S,12aR)-八氢-3,6,9-三甲基-3,12-桥氧-12H-吡喃〔4,3-j〕-1,2-苯并二塞平-10(3H)-酮。分子式为C15H22O5,属倍半萜内酯,具有过氧键和6-内酯环,有一个包括过氧化物在内的1,2,4-三噁结构单元,这在自然界中十分罕见,分子中包括有7个手性中心,它的生源关系属于amorphane类型,其特征是A,B环顺联,异丙基与桥头氢呈反式关系。 制备熔点为156-157℃,[a]D17=+66.3°(C=1.64氯仿)。易溶于氯仿、丙酮、乙酸 青蒿素的化学结构(2张) 制备 化学合成 化学合成青蒿素难度极大,1986年,中国科学院上海有机所以R(+)一香草醛为原料合成了青蒿素,国外也有类似工作,反应以(-)- 2-异薄勒醇为原料,通过光氧化反应引进过氧基,保留原料中的六元环,环上三条侧链烷基化,形成中间体,最后环合成含过氧桥的倍半萜内酯。但过程均过于复杂,尚未显示出商业的可行性。[23-25] 青蒿素化学合成途径
生物合成 萜类化合物的生物合成途径非常复杂,对于青蒿素这一类低含量的复杂分子的生物合成研究更是如此。用以下三种途径可生物合成青蒿素:(1)通过添加生物合成的前体来增加青蒿素的含量;(2)通过对控制青蒿素合成的关键酶进行调控,或者对关键酶控制的基因进行激活来大幅度增加青蒿素的含量;(3)利用基因工程手段来改变关键基因以增强它们所控制酶的效率。[26] 对于倍 青蒿素生物合成途径 半萜内酯的合成,其限速步骤一是环化和折叠成倍半萜母核的过程,另一个限速步骤为形成含过氧桥的倍半萜内酯过程。研究人员通过放射性元素示踪法对青蒿素的生物合成途径进行了研究,认为青蒿素的生物合成可以从法尼基焦磷酸出发,经耗牛儿间架(germacrane)、双氢木香交酯(dihydrocostunodile)、杜松烯内酯(cardinanolide)和青蔷素B(arteannuin B),最终合成青蒿素。[27-28] 除青蒿,其他植物并非不可行。2011 年研究人员使用甲羟戊酸,从烟草中合成出了青蒿素。 [29] 提取