European U rology
European Urology 44(2003)549–555
BPH and Inflammation:Pharmacological Effects of Permixon on Histological and Molecular Inflammatory Markers.Results of a Double Blind Pilot Clinical Assay
R.Vela Navarrete a,*,J.V .Garcia Cardoso a ,A.Barat b ,F.Manzarbeitia b ,A.Lo
′pez Farre ′c a
Department of Urology,Fundacio
′n Jime ′nez D?′az,Universidad Auto ′noma,6Avda.Reyes Catolicos,2,28040Madrid,Spain b
Department of Pathology,Fundacio
′n Jime ′nez D?′az,Universidad Auto ′noma,Madrid,Spain c
Department of Molecular Biology,Fundacio
′n Jime ′nez D?′az,Universidad Auto ′noma,Madrid,Spain First published online 29July 2003
Abstract
Introduction:The role of in?ltrating cells (I.C.),commonly observed in the adenoma interstitial tissue,is unknown.We tested the hypothesis that I.C.are related with BPH progression by:phenotypically characterising these cells;quantifying the expression of lymphokines and growth factors;investigating the response to Permixon (P)in a clinical study.Permixon is a Lipido Sterolic Extract of Serenoa repens possessing pharmacological activities and widely used in the treatment of men with BPH.
Material and Methods:A multicenter open pilot study of two parallel groups on BPH patients was carried out.They were randomized to receive either oral Permixon (P)160mg bid for three months or to be followed for 3weeks without any treatment before surgery (control group C).Strict inclusion and exclusion criteria were applied to conform homogeneous groups,avoiding interferences of in?ammatory drugs or others.Baseline clinical pro?le was almost identical in both groups in terms of age (65:7?5:1vs.67:1?5:8years),IPSS (19:8?6:1vs.19:0?5:8),prostate volume (64:8?18:9vs.71:5?29:3cc),Q max (9:6?3:2vs.10:6?2:6ml/s),and Q L (4:0?1:1vs.3:5?0:7).Surgery was ultimately performed on 29patients (17C,12P)by TURP or retropubic adenomectomy.Adenoma samples were routinely stained with HE and later prepared for immunohistochemical studies using CD3,CD20and CD68antibodies.Counting of positives cells,lymphoid aggregates and foci were done using EnVision technique and the Tech Mate processor.Cytokines,growth factors and eicosanoids were determined by Elisa kits following the manufactured recommendation.
Results:Histological:A difference was observed in the number of lymphocytes B between C (91:4?44:1)and P treated (58:2?53:7)groups (p ?0:097).Biological markers:TNF a and IL-1b were dramatically lower in the Permixon treated group.Other parameters did not show signi?cant changes.Clinical:IPSS in the Permixon treated group was signi?cantly reduced (p <0:006)from 20:0t5:9to 14:9t3:8after three months of https://www.doczj.com/doc/fc6127792.html,ments:The BPH in?ammatory hypothesis was tested in humans.Our pilot study shows a signi?cant reduction of some in?ammatory parameters in prostatic tissues of patients treated with Permixon.These biological ?ndings justify a pharmacological effect of this drug on the in?ammatory status of the adenoma.A correlation with clinical improvement was observed.
#2003Elsevier B.V .All rights reserved.
Keywords:Serenoa repens;Permixon;In?ammation;BPH
1.Introduction
The presence of mononuclear cells in?ltrating the interstitium of BPH tissue,unlike normal prostate tissue,is an old,common and well-documented observation
*
Corresponding author.Tel.t34-91-549-66-56.
E-mail address:rvela@fjd.es (R.Vela Navarrete).
0302-2838/$–see front matter #2003Elsevier B.V .All rights reserved.
doi:10.1016/S0302-2838(03)00368-3
[1–5].In the past it was considered that this leucocyte in?ltration,mainly formed by lymphocytes and macro-phage cells,typical representatives of a chronic in?am-matory process,had some relation with BPH genesis[2]. Only recent studies have tried to phenotypically identify these cells and to discover the biological meaning of their presence in the adenoma interstitial tissue both in human[6–8]and in animal models[9].Do they have a role in the genesis and progression of the BPH?Or,do they only represent an unspeci?c reaction to mechanical dif?culties and obstruction in the BPH acinis?What markers,in?ammatory or other,are expressed by these cells?
Current knowledge admits the hypothesis that acti-vation of mononuclear cell population in a particular focus induces two different kinds of response:through cytokine release,the secretion of some growth factors
and,through the release of some membrane phospho-lipids,the increased synthesis of in?ammatory media-tors such as prostaglandins and leukotrienes[10–12]. The enzymes responsible for the latter reaction are phospholipase A2,cyclooxigenase and lipoxigenase.In the case of BPH most pieces of this hypothetical sequence are still lacking?rm evidence.
The following clinical trial was designed to answer some of these queries and simultaneously investigate how Permixon,a lipido sterolic extract of Serenoa repens widely used in the treatment of men with lower urinary tract symptoms suggestive of BPH,affects the in?ammatory markers potentially involved in this process.
2.Material and methods
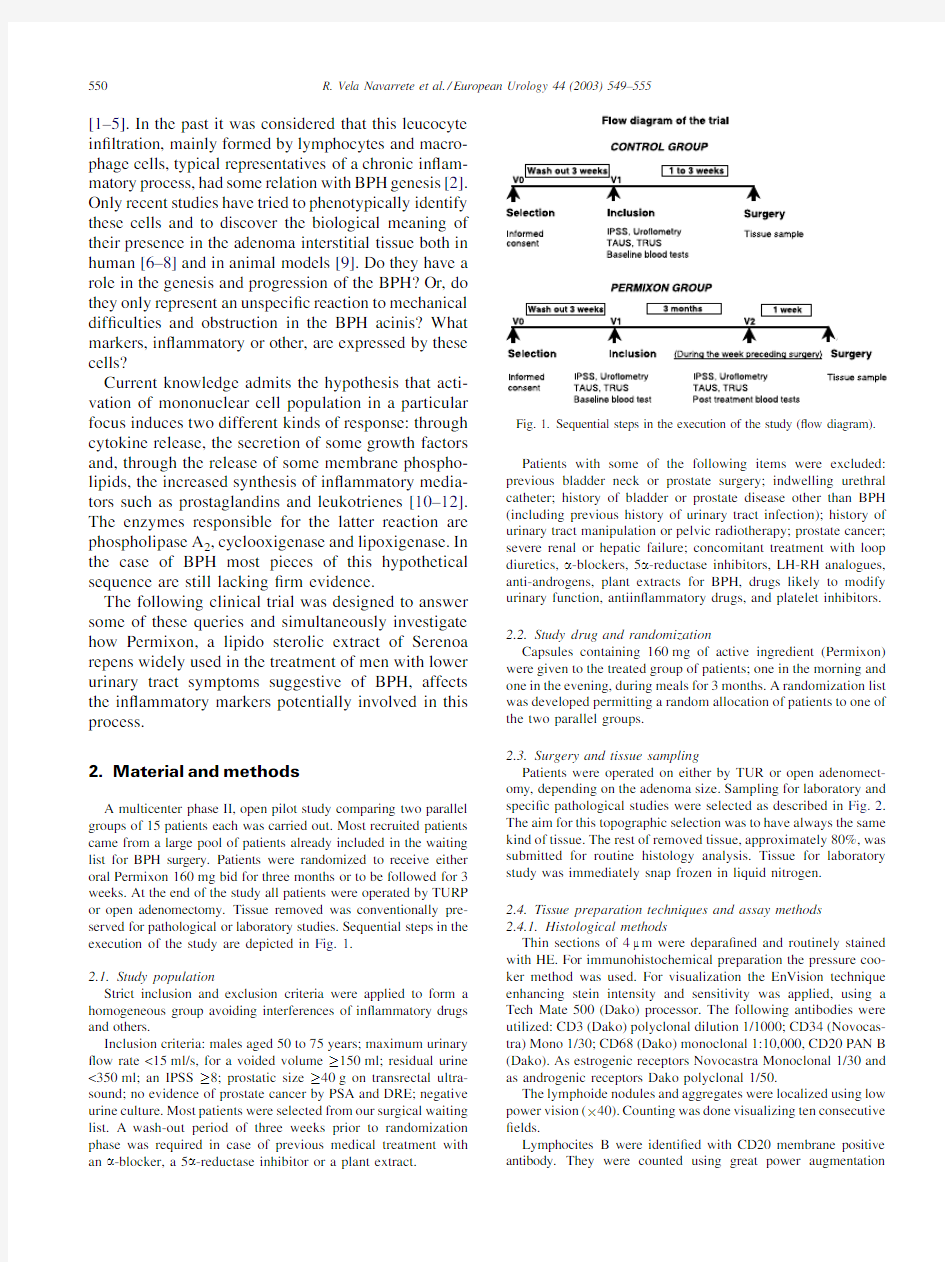
A multicenter phase II,open pilot study comparing two parallel groups of15patients each was carried out.Most recruited patients came from a large pool of patients already included in the waiting list for BPH surgery.Patients were randomized to receive either oral Permixon160mg bid for three months or to be followed for3 weeks.At the end of the study all patients were operated by TURP or open adenomectomy.Tissue removed was conventionally pre-served for pathological or laboratory studies.Sequential steps in the execution of the study are depicted in Fig.1.
2.1.Study population
Strict inclusion and exclusion criteria were applied to form a homogeneous group avoiding interferences of in?ammatory drugs and others.
Inclusion criteria:males aged50to75years;maximum urinary ?ow rate<15ml/s,for a voided volume!150ml;residual urine <350ml;an IPSS!8;prostatic size!40g on transrectal ultra-sound;no evidence of prostate cancer by PSA and DRE;negative urine culture.Most patients were selected from our surgical waiting list.A wash-out period of three weeks prior to randomization phase was required in case of previous medical treatment with an a-blocker,a5a-reductase inhibitor or a plant extract.
Patients with some of the following items were excluded: previous bladder neck or prostate surgery;indwelling urethral catheter;history of bladder or prostate disease other than BPH (including previous history of urinary tract infection);history of urinary tract manipulation or pelvic radiotherapy;prostate cancer; severe renal or hepatic failure;concomitant treatment with loop diuretics,a-blockers,5a-reductase inhibitors,LH-RH analogues, anti-androgens,plant extracts for BPH,drugs likely to modify urinary function,antiin?ammatory drugs,and platelet inhibitors.
2.2.Study drug and randomization
Capsules containing160mg of active ingredient(Permixon) were given to the treated group of patients;one in the morning and one in the evening,during meals for3months.A randomization list was developed permitting a random allocation of patients to one of the two parallel groups.
2.3.Surgery and tissue sampling
Patients were operated on either by TUR or open adenomect-omy,depending on the adenoma size.Sampling for laboratory and speci?c pathological studies were selected as described in Fig.2. The aim for this topographic selection was to have always the same kind of tissue.The rest of removed tissue,approximately80%,was submitted for routine histology analysis.Tissue for laboratory study was immediately snap frozen in liquid nitrogen.
2.4.Tissue preparation techniques and assay methods
2.4.1.Histological methods
Thin sections of4m m were depara?ned and routinely stained with HE.For immunohistochemical preparation the pressure coo-ker method was used.For visualization the EnVision technique enhancing stein intensity and sensitivity was applied,using a Tech Mate500(Dako)processor.The following antibodies were utilized:CD3(Dako)polyclonal dilution1/1000;CD34(Novocas-tra)Mono1/30;CD68(Dako)monoclonal1:10,000,CD20PAN B (Dako).As estrogenic receptors Novocastra Monoclonal1/30and as androgenic receptors Dako polyclonal1/50.
The lymphoide nodules and aggregates were localized using low power vision(?40).Counting was done visualizing ten consecutive ?elds.
Lymphocites B were identi?ed with CD20membrane positive antibody.They were counted using great power
augmentation Fig.1.Sequential steps in the execution of the study(?ow diagram).
550R.Vela Navarrete et al./European Urology44(2003)549–555
(?400)in 3or 5?elds depending of the homogeneity of the in ?ltrate.A similar procedure has been used for counting lymphocytes T (CD3positive cells).The sum of these three groups of cells mean constitute the number of mononuclear cells in ?ltrating the interstitium.2.4.2.Assay methods
Cytokines,growth factors and eicosanoids were determined by Elisa kits following the manufactured recommendations,COX-2and iNOS expression was determined by Western blot.For this purpose,samples were pulverized and the proteins resuspended in Laemmli buffer containing mercaptoethanol.Proteins were sepa-rated in 10%SDS-PAGE electrophoresis.Then,the gel was trans-ferred to nitrocellulose and hibridated with monoclonal antibodies against iNOS and COX-2.After,a second antibody (horsedish peroxidase-conjugated antibody)was added.Speci ?c COX-2and iNOS protein were evaluated by enhanced chemiluminiescence.2.5.Evaluation criteria
Clinical evaluation in the treated group was done using the following measuring instrument:IPSS (global score determined at inclusion and after treatment);uro ?owmetry (Urodyn 1000,Dan-tec)with maximum ?ow rate (Q max )and mean ?ow rate (Q aver );residual urine volume (transabdominal sonography).
Histological:Adenoma in ?ltration by lymphocytes and leuco-cytes was evaluated in terms of changes in the number and quality of lymphocytes and the number and quality of leucocytes.
Laboratory evaluation:Tissue concentration in leucotrienes,prostaglandines,growth factors and cytoquines was evaluated in terms of changes of the parameters listed in Table 3.
2.6.Statistical methods and analyses
Statistical analysis was carried out by statitec,using the SAS package (version 6.07,VM/CMS environment).Initial clinical comparison between the two groups was made by means of the following tests:Student test for ‘‘continuous ’’variables;Wilcoxon rank sum test for ordinal variables;and w 2-test for non-ordered categorical variables.For the analysis of prostatic tissue parameters,IPSS and urodynamic parameters comparison by the Student ’s t -test was used when the distribution was normal,or not far from a normal law,and by a Wilcoxon ’s rank sum test in other cases.
3.Results
A total of 46patients were enrolled,35were selected,19of them in the control arm and 16
in
Fig.2.Sampling for laboratory and speci ?c pathological studies.Notice that tissue was obtained from the same zone of the adenoma both in TURP and retropubic adenomectomy.
R.Vela Navarrete et al./European Urology 44(2003)549–555551
the Permixon group.Six patients dropped out for different reasons:four of them in the Permixon group and 2in the control group.Finally 29patients were operated (17control/12Permixon)either by TURP (17)or open adenomectomy (12).
3.1.Clinical results
Both groups of patients had a similar pro ?le for age (65:7?5:1vs.67:1?5:8),prostate volume (64:8?18vs.71:5?29cc),Q max (9:6?3:2vs.10:6?2:6),IPSS (18:8?6:1vs.19:0?5:9),Q L (4:0?1:1vs.3:5?0:8)and other general health status variants (Table 1).
A 5.1point reduction in the IPSS score was observed in the Permixon treated group between V 1and V 2with a p value of 0.006(Table 2and Fig.3).The individual analysis of symptoms showed a signi ?cant reduction (p <0:044)in the IPSS question number 1related to the sensation of emptying the bladder.There was a signi ?cant reduction when obstructive (p ?0:04)and irritative (p ?0:05)symptoms were separately compared between V 1and V 2.There was no signi ?-cant modi ?cation in the uro ?owmetric parameters,in prostate volume or in PSA levels after 3months ’treatment.
3.2.Histological ?ndings and results
As shown in Table 3and Fig.4there were no signi ?cant differences between control group and trea-ted patients in the number of lymphocyte nodules and aggregates,as in the number of total interstitial mono-nuclear cells,T lymphocites and macrophages.How-ever a more signi ?cant difference in the number of B lymphocites,(94:4?44:1vs.58:2?53:7)could be observed,with a reduced ?gure in the treated
tissue.
T able 1
T able 2
Fig.3.Clinical results:clinical pro ?le of control and treated patients at V 1and V 2.Signi ?cant reduction of IPSS (p ?0:006)in the treated group.
552R.Vela Navarrete et al./European Urology 44(2003)549–555
https://www.doczj.com/doc/fc6127792.html,boratory results
3.3.1.Representatives of the arachidonic acid cascade
COX-2varied from 32.2to 99.5pg/mg with an mean value of 59:4?21:9.No signi ?cant differences were observed with the treated values (65:9?19:6).A simi-lar pattern has been obtained with iNOS (79:9?33:4vs.86:0?47:6)and other measured markers such as LTB4(36:8?8:3vs.46:4?14:3)(Table 3).
3.3.2.Cytokines and growth factors
TNF a and IL-1b showed high values in the control group (628:6?635:5and 38:1?3:1pg/mg protein)with a dramatic reduction in the Permixon treated group (146:9?87:3,p ?0:012and 18:1?9:8,p ?0:004)for TNF a and IL-1b respectively (Figs.5and 6).However no signi ?cant changes were observed in IL-6,TGF b or EGF.
4.Discussion
BPH in ?ammatory hypothesis has been tested in humans in an open randomized pilot study,evaluating simultaneously the antiin ?ammatory effects of Per-mixon,a drug with potential antiin ?ammatory bene ?ts as reported in previous ‘‘in vitro ’’studies [10,11],and widely used in the treatment of BPH [13,14].The objectives of this study were the following:(1)To de ?ne the histological in ?ammatory patterns more commonly observed in patients with mature adenomas.(2)To categorize and identify the mononuclear cells in ?ltrating the adenoma tissue.(3)To compare changes in number and nature of these cells in patients treated with Permixon.(4)To identify biological markers most representatives of the potential in ?ammatory process and its changes when treated by Permixon.
Mononuclear cell in ?ltration of the adenoma tissue is a well-documented observation [1–5].Contrary to the traditional view,viz.that in ?ltrates develop in response to bystander chronic infection and have no relevant impact on BPH development,these in ?ltrates
T able 3
Number of total interstitial mononuclear cells and molecular markers included in this study,with average ?ndings in control group,treated group and changes observed (p value)
Control (Mean ?S.D.)Permixon (Mean ?S.D.)
p value a Total number of in ?ltrates 149.3?61.4111.3?52.40.120B lymphocytes 91.4?44.258.2?36.80.087T lymphocytes 46.4?19.143.1?17.20.661Macrophages
11.5
?7.0
9.95
?2.1
0.833Interleukine 1(pg/mg protein)38.5?18.318.1?9.90.004Interleukine 6(pg/mg protein)2255?22753037?27410.133TNF a (pg/mg protein)628.6?635.5146.9?87.30.012TGF b (pg/mg protein) 6.4?3.1 5.1?2.90.408EGF (pg/mg protein)17.51?12712.1?5.90.307COX-2(UA)59.4?21.965.9?19.60.449LTB4(UA)36.8?8.246.4?14.30.128iNOS (UA)
76.9?33.3
86.1?47.5
0.570
Lymphocites B were reduced in 36.2%(p ?0:09).a
Student or Wilcoxon rank
test.
Fig.4.Pathological results:no signi ?cant differences were observed in the number of total interstitial mononuclear cells,T lymphocites and macro-phages.However,B lymphocites were reduced in 36.2%(p ?0:
09).
Fig.5.Levels of interleukine 1b in prostate tissue samples taken from control and Permixon treated
patients.
Fig.6.Changes in biological markers:a 3-month treatment with Permixon produces a potent and signi ?cant decrease in prostatic cytokines IL-1b (à54%vs.control,p ?0:004)and TNF a (à77%vs.control,p ?0:012).Moreover,there is a good correlation between IL-1and TNF a content,thus validating the dosages.
R.Vela Navarrete et al./European Urology 44(2003)549–555
553
lack signi?cant numbers of granulocytes.Theyer et al. (1992)[7]and Steiner et al.(2001)[8]have shown that this multifocal increase of leukocytes is due in parti-cular to activated CD4tT lymphocytes.Further, Bierhoff et al.(1996)[15]demonstrated that the increase of diffusely scattered T lymphocyte in?ltra-tion in?broblastic,?bromuscular and smooth muscular stromal nodules,when compared to surrounding stroma,is statistically signi?cant.
Our study con?rms that diffuse in?ltration is the most common pattern,although the presence of nodules is a prominent?nding in other cases.Both patterns may coexist.In the?rst case the cell distribu-tion affects the whole interstitial space,with more or less homogeneity.The nodules are mainly localized in the extraglandular area.Average of in?ltrating cells was 149:3?61:4in the control group and111:3?52:4in the treated group,with a reduction of25%.The number of in?ammatory nodules was similar in both groups (6:4?3:4in the control group and7:6?3:9in the treated group).
The absence of granulocytes was also con?rmed in this study.Most of the cells located in the interstitium were CD20t,showing some discordance with pre-viously reported studies[7,8],while the nodule popu-lation were CD3t.The most signi?cant observation after treatment was a36.24%reduction of CD20tcells.The whole cell count,which represents the sum of CD3t,CD20tand,CD68twas reduced to a lesser extent(25%).
The presence and levels of in?ammatory markers in the adenoma tissue in humans(not in the whole prostate tissue)have been rarely investigated.Steiner et al.(2001)[16]have demonstrated that IL-2,IL-4, IL-13,TGF b and IFN g are increased,being the T lymphocytes the main source of its production. Handisurya et al.(2000)[17]and Stix et al.(2001) [18]have con?rmed an important increase of IL-15and IFN g.Increase of EGF in adenomatous tissue has been demonstrated by di Siverio et al.(1998)[19]and de Miguel et al.(1999)[20].Other growth factors have been also investigated[21].
We have observed that the treatment with Permixon causes a variable and inconsistent response on in?am-matory markers related with the arachidonic cascade, with a slight increase of COX-2,iNOS,and LTB-4. Much more signi?cant have been the changes in TNF a and IL-1b,with a dramatic decrease ofà76%and à36%respectively.In accordance with that there was also a decreasing tendency in the levels of EGF (à31%),TGF b(à12%)but not in IL-6(t18%). The role of IL-1b and TNF a in in?ammatory processes is well known[22]and both biological markers have been used as indicators of prostatic in?ammation when increased in prostatic secretion in cases of chronic prostatitis(Nadler et al.,2000[23]).IL-1b increase also has been demonstrated in in?ammatory prostatic cell line by Klein et al.(1997)[24].
It is dif?cult to hypothesize on the role of in?am-mation in the genesis and maturation of prostate ade-noma in the light of our current data.However, histological and molecular?ndings suggest a determi-nant participation of in?ammation in BPH natural history,independently of the precise mechanisms and actors participating in this process.Mononuclear cell in?ltration of the adenoma is not an unspeci?c reaction due to mechanical glandular secretion dif?-culties or other.On the contrary,it represents a chronic in?ammatory process with tissue and systemic con-sequences[25,26].Our pilot study recognizes IL-1b and TNF a as being the most prominent in?ammatory biological markers.A3-month treatment with the Lipido Sterolic extract of Serenoa repens(Permixon) produces a signi?cant reduction of these cytokines, coincidently with a reduction in prostatic interstitial B lymphocytes and a signi?cant clinical improvement. We can reasonably speculate that Permixon modi?es the in?ammatory status of BPH tissue through cytokine regulation.
Acknowledgements
The authors thank the collaboration received from the following institutions and doctors:Ciudad Sanitaria Pr?′ncipes de Espan?a,Barcelona(Drs.N.Serrallach;N. Camps,F.Vigues,E.Condom*).Hospital Cl?′nico y Provincial,Barcelona(Drs.P.Carretero;A.Franco, Ferna′ndez*).Hospital Mu′tua de Terrasa,Barcelona (Drs.J.Ristol,JM.Caballero;LL Marti,Sala*).Hos-pital Doctor Peset,Valencia(Drs.FJ.Vidal Moreno; JR Beltran;V.Rodrigo; A.Cremades*).Hospital Municipal de Badalona,Barcelona(Drs.FJ.Blasco, S.Bucar,M.Gomez*)(*:anatomo-pathologists).
References
[1]Moore RA.In?ammation of the prostate gland.J Urol1937;38:173.
[2]Moore RA.Benign hypertrophy of the prostate.A morphological
study.J Urol1943;50:680–710.[3]Kohnen PW,Drach GW.Patterns of in?amation in prostatic
hyperplasia:a hystologic and bacteriologic study.J Urol1979;121: 755–60.
554R.Vela Navarrete et al./European Urology44(2003)549–555
[4]Helpap B.Pathologie der chronischen unspezi?schen Prostatitis.In:
Vahlensieck W,Rutishauser G,editors.Benigne Prostatopathien.
Stuttgart:Thieme;1992.p.35–50.
[5]Helpap B.Histological and immunohistochemical study of chronic
prostatic in?ammation with and without bening prostatic hyperpla-sia.J Urol Pathol1994;2:49–64.
[6]McClinton S,Miller ID,Eremin O.An immunohistochemical
characterisation of the in?ammatory cell in?ltrate in bening and malignant prostatic disease.Br J Cancer1990;61:400–3.
[7]Theyer G,Kramer G,Assmann I,Sherwood E,Preinfalk W,
Marberger M,et al.Phenotypic characterization of in?ltrating leukocytes in being prostatic hyperplasia(BPH).Lab Invest 1992;66(1):96–106.
[8]Steiner RG,Marberger M.Characterization of BPH in?ltrating T
lymphocytes regarding phenotype.J Urol2001;165:26.
[9]Mahapokai W,van den Ingh TSGAM,van Mil F,van Garderen E,
Schalken JA,Mol JA,et al.Immune response in hormonally-induced prostatic hyperplasia in the dog(Thesis).Utrecht;2000.
[10]Ragab A,Ragab-Thomas JMF,Delhon A,Tisne-Versailles J,
Gassama-Diagme A,Fauvel J,et al.Effects of Permixon on phospholopase A2activity and on arachidonic acid metabolism in cultured prostatic cells.Acta Me′d1998;293–6.
[11]Plaubert-Braquet M,Mencia Huerta JM,Cousse H,Braquet P.
Effect of the lipidic lipidosterolic extract of Serenoa repens (Permixon)on the ionophore A23187-stimulated production of leukotriene B4(LTB4)from human polymophonuclear neutrophils.
Prostaglandins,Leukotrienes and Essential Fatty Acids1997;57(3): 299–304.
[12]Stewart RJ,Panigraphy D,Flynn E,Folkman J.Vascular endothelial
growth factor and tumor angiogenesis are regulated by androgens in hormone responsive human prostate carcinoma:evidence for androgen dependent destabilization of vascular endothelial growth factor transcripts.J Urol2001;165(2):688–93.
[13]Carrao JC,Raynaud JP,Koch,et https://www.doczj.com/doc/fc6127792.html,parison of phytotherapy
(Permixon)with?nasteride in the treatment of bening prostatic hyperplasia:a randomised international study of1,098patients.
Prostate1996;29(4):231–40.
[14]Debruyne F,Koch G,Boyle P,Calais Da Silva F,Gillenwater J,
Hamdy F,et https://www.doczj.com/doc/fc6127792.html,parison of a phytotherapeutic agent(Permixon) with an alpha-blocker(tamsulosin)in the treatment of benign prostatic hyperplasia:a1-year randomized international study.Eur Urol2002;41:497–507.[15]Bierhoff E,V ogel J,Benz M,Giefert TH,Wernert N,Pfeifer U.
Stromal nodules in Bening Prostatic Hyperplasia.Eur Urol1996;
29:345–54.
[16]Steiner RG,Mamaran-Dadgar N,Langer D,Maderbacher S,
Reithmayer F,Marberger M.Characterization of BPH autoantigens that differentiate between Finasteride responders and non-respon-ders.J Urol2001;165:213.
[17]Handisurya A,Stix U,Ecker RCh,Pfaffenede-Mantai S,et al.
Differential expression of IL-15,a proin?ammatory and anti-apoptotic cytokine and its receptor in human prostate.J Urol2001;165:209. [18]Stix U,Ecker R,Pfaffeneder-Mantai S,Langer D,Kramer G,
Memaran-Dadgar N,et al.Differential expression of interleukin-15,
a proin?ammatory and anti-apoptotic cytokine and its receptor in
human prostate.J Urol2001;165(5).
[19]Di Silveiro F,Monti S,Sciarra A,Varasano PA,Martini C,Lanzara S,
et al.Effects of long term treatment with Serenoa Repens(Permixon) on the concentrations and regional distribution of androgens and epidermal growth factor in BPH.Prostate1998;37(2):77–83. [20]De Miguel MP,Royuela M,Bethencourt FR,Ruiz A,Fraile B,
Paniagua R.Inmunohistochemical comparative analysis of trans-forming growth factor a,epidermal growth factor,and epidermal growth factor receptor in normal,hyperplastic and neoplastic human prostates.Cytokine1999;9:722–7.
[21]Lawson RK.Growth factor and benign prostatic hyperplasia.Wld J
Urol1989;6:190–3.
[22]Feghali CA,Wright TM.Cytokines in acute and chronic in?amma-
tion.Frontiers in Bioscience1997;2:12–26.
[23]Nadler RB,Koch AE,Clahoun EA,Campbell PL,Pruden DL,
Bennett CL,et al.IL-1beta and TNF-alpha in prostatic secretions are indicators in the evaluation of men with chronic prostatitis.J Urol 2000;164(1):214–8.
[24]Klein RD,Borchers AH,Sundareshan P,Bougelet C,Berkman MR,
Nagle RB,et al.Interlukin-1beta secreted from monocytic cells induces the expression of matrilysin in the prostatic cell line LNCaP.
J Biol Chem1997;272(22):14188–92.
[25]Perez Blas M,Martinez-Martin B,Carballido J,Hontoria J,Salazar L,
Olivier C,et al.Defective functional response to membrane stimule in lymphocytes from patients with BPH.Clin Exp Inmunol1995;101:521.
[26]Elsa¨sser-Beile U,Przytulsky B,Gierschner https://www.doczj.com/doc/fc6127792.html,parison of the
activation status of tumor in?ltrating and peripheral lymphocytes of patiens with adenocarcinomas and benign hyperplasia of the prostate.
Prostate2000;45:1–7.
R.Vela Navarrete et al./European Urology44(2003)549–555555
药物临床试验安全评价·广东共识(2020年版) 广东省药学会2020年8月1日发布 更新说明 药物临床试验过程中对药物安全性进行评价,是全面、客观评价一个试验 药物不可或缺的内容。新版《药物临床试验质量管理规范》(GCP)中,强调 了申办者在安全性信息收集、评价、递交和分发环节中的责任,也对研究者如 何保障受试者安全、做好安全信息记录和评价提出了更为明确的要求。本共识 旨在为研究者进行安全性信息的收集、评价、递交提供指导,为申办者理解研 究者的相关工作细节和制定安全信息收集要求提供参考。 为规范和帮助药物临床试验中安全性评价工作,广东省药学会药物临床试 验专业委员会分别于2016年和2018年发布了《药物临床试验安全评价?广东共识》供同行参考。随着共识的推广与运用,得到很多业内同行的关注与好评, 也不断收到一些完善建议。2020年7月1日,国家药品监督管理局与国家卫 生健康委发布的新版《药物临床试验质量管理规范》(GCP)(以下简称新版GCP)正式实施,对研究各方在安全性信息收集、评价、递交与分发方面的权 责进行了更为详细的规定,体现了中国临床试验监管与时俱进,与ICH-GCP 全面接轨的决心和行动力。 安全评价,作为药物临床试验中研究各方共同关注的评价内容,实施中尚 有一些实操环节需明确和共同遵循的做法。本次更新主要遵照新版GCP结合 国家药监局药品审评中心《药物临床试验期间安全性数据快速报告的标准和程
序》,对相关定义进行全面梳理,对章节框架进行调整,力求更为清晰和增强 逻辑性,保持共识的生命力,成为一份与时俱进的行业共同认识。 本次修订得到专委会各位专家的指导,在此向各位专家的无私付出表示衷心感谢! 共识撰写小组2020年7月14日 目录 一总则二定义 2.1 不良事件 2.2 严重不良事件 2.3 重度不良事件与严重不良事件 2.4 药物不良反应 2.5 可疑且非预期严重不良反应 2.6 重要不良事件 2.7 治疗期出现的不良事件 2.8 特别关注的不良事件 三不良事件/严重不良事件的收集、记录、描述 3.1 不良事件名称的确定 3.2 不良事件的开始时间 3.3 不良事件的随访 3.4 不良事件的结束时间
药物临床试验期间安全性数据快速报告标准和程序 为落实原国家食品药品监督管理总局《关于适用国际人用药品注册技术协调会二级指导原则的公告》(2018年第10号)的要求,我中心依据ICH药物警戒相关指导原则【E2A、E2B(R3)和M1】,起草了《药物临床试验期间安全性数据快速报告标准和程序》(以下称“本标准和程序”),具体如下: 一、申请人获准开展药物(包括化药、中药及生物制品)临床试验后,对于临床试验期间发生的(包括中国境内和境外)所有与试验药物肯定相关或可疑的非预期且严重的不良反应(以下简称“非预期严重不良反应”),以及本标准和程序规定的其它情形,都应按照本标准和程序在规定的时限内向国家药品审评机构进行快速报告。 二、严重不良反应指以下情形之一:(1)导致死亡;(2)危及生命,指严重病人即刻存在死亡的风险,并非是指假设将来发展严重时可能出现死亡;(3)导致住院或住院时间延长;(4)永久或显著的功能丧失;(5)致畸、致出生缺陷;(6)其他重要医学事件:必须运用医学和科学的判断决定是否对其他的情况加速报告,如重要医学事件可能不会立即危及生命、死亡或住院,但如需要采取医学措施来预防如上情形之一的发生,也通常被视为是严重的。例如在急诊室的重要治疗或在家发生的过敏性支气管痉挛,未住院的恶液质
或惊厥,产生药物依赖或成瘾等。 三、非预期不良反应指不良反应的性质、严重程度、后果或频率,不同于试验药物当前相关资料(如研究者手册等文件)所描述的预期风险。研究者手册作为主要文件提供用以判断某不良反应是否预期或非预期的安全性参考信息。如:(1)急性肾衰在研究者手册中列为不良反应,但试验过程中出现间质性肾炎,即应判断为非预期不良反应,(2)肝炎在研究者手册中列为不良反应,但试验过程中发生急性重型肝炎,即应判断为非预期不良反应。 四、申请人在药物临床试验期间,判断与试验药物肯定相关或可疑的非预期且严重的不良反应,均需要按本标准和程序以个例安全性报告的方式快速报告。 申请人和研究者在不良事件与药物因果关系判断中不能达成一致时,其中任一方判断不能排除与试验药物相关的,也应该进行快速报告。 五、以下情况一般不作为快速报告内容:(1)非严重不良事件;(2)严重不良事件与试验药物无关;(3)严重但属预期的不良反应;(4)当以严重不良事件为主要疗效终点时,不建议申请人以个例安全性报告(ICSR)形式向国家药品审评机构报告。 六、阳性对照药相关的严重不良反应,申请人有责任决定是否向其他的药品生产商和/或直接向国家药品监督管理
中国肺癌杂志2014年3月第17卷第3期 Chin J Lung Cancer, March 2014, Vol.17, No.3 ·综述· 非小细胞肺癌免疫治疗进展 何圆 尤长宣 【摘要】 肺癌是全球范围内癌性死亡的首要因素,发病率、死亡率高,预后较差,急需开发一种新的高效低毒疗法。作为术后辅助或是姑息治疗手段,免疫治疗为非小细胞肺癌患者提供了一个新的治疗方向。免疫疗法作用机理各不相同,如免疫检测点受体抑制剂(抗CTLA4抗体、抗PD-1抗体、抗PD-L1抗体)、主动性免疫疫苗(L-BLP25脂质体疫苗、Belagenpumatucel-L 疫苗、MAGE-A3蛋白疫苗)、过继性免疫疫苗(CIK 细胞)等,研究表明免疫治疗非小细胞肺癌肿瘤缓解率较前提高,前景值得期待,II 期/III 期临床试验亦在进一步探索其临床应用价值。本文就当前非小细胞肺癌免疫疗法原理、临床试验、不良反应及待解决问题作一概述。 【关键词】 肺肿瘤;免疫治疗;进展 Advances in Immunotherapies for Non-small Cell Lung Cancer Yuan HE 1 , Changxuan YOU 2 1 Graduate Student of Southern Medical University, Guangzhou 510515, China; 2Department of Oncology, Nanfang Hospital, Southern Medical University, Guangzhou 510515, China Corresponding author: Changxuan YOU, E-mail: ycx6026@https://www.doczj.com/doc/fc6127792.html, 【Abstract 】 Globally, Lung cancer is the leading cause of cancer-related death of high morbidity and mortality with poor prognosis, which needs some more effective and less toxic therapies. The immunotherapies offer a novel approach for the treatment of patients with non-small cell lung cancer (NSCLC) in both the adjuvant and palliative disease settings. A number of promising immunotherapies based on different mechanism have now been evaluated showing an increasing response rate. Moreover, further phase II/III clinical trials will be indicated to explore its value. These include checkpoint inhibitors (anti-CT-LA4 antibody, anti-PD-1 antibody, anti-PD-L1 antibody), active vaccination (L-BLP25 liposome vaccine, Belagenpumatucel-L vaccine, MAGE-A3 protein vaccine) and adoptive vaccination (CIK cells). The purpose of this paper will draw a summary on the theory, clinical trials, toxicity and problems to be solved of the immunotherapies in NSCLC. 【Key words 】 Lung neoplasms; Immunotherapies; Progress This study was supported by the grants from National Natural Science Foundation of China (No.81071847), Guangdong Natural Science Foundation (No.S2011010003881), Guangdong Provincial Science and Technology Project (No.2012B031800394), Wu Jieping Medical Foundation Funded Special Clinical Research Projects (No.320.6799.1118)(all to Changxuan YOU). DOI: 10.3779/j.issn.1009-3419.2014.03.17 本研究受国家自然科学基金项目(N o.81071847)、广东省自然科学基金项目(No.S 2011010003881)、广东省科技项目(No.2012B031800394)和吴阶平医学基金会临床科研专项资助项目(No.320.6799.1118)资助 作者单位:510515 广州,南方医科大学2013级研究生(何圆);510515 广州,南方医科大学南方医院肿瘤科(尤长宣)(通讯作者:尤长宣,E-mail: ycx6026@https://www.doczj.com/doc/fc6127792.html, ) 肺癌是全球范围内首个癌症相关性死亡因素,非小细胞肺癌(non-small cell lung cancer, NSCLC )约占肺癌总数80%-85%,吸烟、环境污染(厨房油烟、煤炭燃烧、汽车尾气)等构成肺癌发病的主要原因。早期接受治疗NSCLC 患者超过40%会出现肿瘤复发,因此晚期 NSCLC 患者5年生存率不到15%,预后较差[1]。以铂类为基础的标准化疗方案治疗NSCLC ,患者肿瘤缓解率仅为20%-35% ,中位生存期(median overall survival, mOS )为10个月-12个月,分子靶向治疗与化疗方案相比,可延长NSCLC 患者无疾病生存期(progression-free survival, PFS ),但患者mOS 未获益[2]。因此标准治疗或因严重不良反应(恶心、呕吐、骨髓毒性等)或因经济学毒性(分子靶向药物价格较昂贵)已使其处于治疗瓶颈水平,急需开发一种新的NSCLC 疗法。目前免疫治疗NSCLC 在I 期/II 期临床试验中结果良好:肿瘤缓解率提高、毒副作用小、患者易耐受,这将为NSCLC 治疗开发新领域。
免疫细胞治疗产品临床试验技术指导原则 (征求意见稿) 国家药品监督管理局药品审评中心 生物制品临床部 2020年7月
目录 一、概述 (3) (一)前言 (3) (二)目的和适用范围 (4) (三)免疫细胞治疗产品的特性 (4) 二、临床试验设计 (6) (一)一般考虑 (6) 1、研究人群 (6) 2、受试者者保护和临床安全性 (9) 3、个体化治疗产品的特殊考虑 (11) (二)探索性临床试验 (12) 1、探索性试验的目的 (12) 2、剂量探索和剂量递增 (13) 3、对照设计 (15) 4、给药间隔 (16) 5、药代动力学(PK)和药效学(PD)研究 (16) (三)确证性临床试验 (17) 1、对照和设盲 (17) 2、疗效和安全性 (18) 三、临床试验结束后研究 (19) (一)临床试验受试者的长期随访 (19) (二)上市后研究或监测 (21) 参考文献 (21)
一、概述 (一)前言 2017年,原国家食品药品监督管理总局发布《细胞治疗产品研究与评价技术指导原则(试行)》,对细胞治疗产品按照药品管理相关法规进行研发时的技术要求进行了总体阐述。该指导原则发布以来,我国细胞治疗产品的研发和注册申报数量明显增加,特别是免疫细胞治疗产品。 免疫细胞治疗是利用人体自身或供者来源的免疫细胞,经过体外培养扩增或活化,再回输到患者体内,激发或增强机体的免疫功能,从而清除肿瘤细胞、病原体或病毒感染等异常细胞的治疗方法,包括过继性细胞治疗(adoptive cell therapy,ACT),治疗性疫苗等。根据作用机制的不同,目前的细胞免疫治疗研究热点类型主要包括:肿瘤浸润淋巴细胞(tumor-infiltrating lymphocytes, TILs)、嵌合抗原受体T细胞(chimeric antigen receptor modified T cells,CAR-T)以及T细胞受体嵌合T细胞(T-cell receptor-engineered T cells,TCR-T)等,此外,还存在基于自然杀伤细胞(natural killer cells,NK)或树突状细胞(dendritic cells,DC)等其它免疫细胞的治疗方法,如细胞因子诱导的杀伤细胞(cytokine-induced killer cells, CIK)等。 当免疫细胞治疗产品进入临床试验时,应遵循《药物临床试验质量管理规范》(GCP)、国际人用药品注册技术协调会(ICH)E6等一般性原则要求。同时,免疫细胞治疗产品的细胞来源、类型、体外操作等方面异质性较大,治疗原理和体内作用等相较传统药物更加复杂。为了获得预期治疗效果,免疫细胞治疗产品可能需要通过特定的手术措施、给药方法或联合治疗
药物临床试验安全评价?广东共识(2018) (广东省药学会2018年4月23日印发) 更新说明 药物临床试验的安全性评价是全面?客观评价一个试验药物不可或缺的内容?安全信息的收集?评价和记录主要由研究者团队完成,但申办者所撰写的研究方案和制定的实施细则是确保高质量信息收集和整理等工作的关键性因素? 为规范和帮助药物临床试验中安全性评价工作,广东省药学会药物临床试验专业委员会于2016年发布了《药物临床试验安全评价?广东共识》供同行参考?随着共识的推广与运用,得到很多业内同行的关注与好评,本专委会也不断收集和整理来自临床实践的困惑点以及业内人士的共识做法,并于2017年8月至2018年3月期间向行业广泛征求修改意见和建议,得到不少热心人士的积极参与,其中部分建议已写入本版共识? 安全评价,作为药物临床试验中研究各方共同关注的评价内容,实施中一直存在尚待明确和共同遵循的做法?本次更新,对之前版本进行了全面梳理,力求不断完善,保持共识的生命力,成为一份与时俱进的行业共识? 本次修订得到本专委会各位专家的指导,特别感谢洪明晃教授对“肿瘤进展是否作为SAE上报”的悉心指导,同时也感谢黄菲霞?赵杏娜等同行在共识征求意见期间提供的宝贵建议和参考依据?在此向各位专家的无私付出表示衷心感谢! 共识撰写小组 2018年4月8日
目 录 1 总则 (3) 2 定义 (3) 2.1 不良事件 (3) 2.2 严重不良事件 (3) 2.3 重度不良事件与严重不良事件 (4) 2.4 可疑的?非预期的严重不良反应 (4) 2.5 重要不良事件 (4) 2.6 治疗后出现的不良事件 (4) 3 不良事件/严重不良事件的收集?记录?描述 (4) 3.1 不良事件名称的确定 (4) 3.2 不良事件的开始时间 (5) 3.3 不良事件的随访 (5) 3.4 不良事件的结束时间 (5) 3.5 不良事件的转归 (5) 3.6 不良事件的合并用药 (5) 3.7 不良事件的严重程度 (6) 3.8 不良事件/严重不良事件的记录与描述 (6) 4 不良事件/严重不良事件的因果关系判断 (6) 4.1 因果关系判断的思路 (7) 4.2 因果关系判断的标准 (7) 4.3 因果关系判断的结果 (7)
阿尔茨海默病免疫治疗的药物临床试验进展 舒 鹤1,牛学才2 (1.济南军区总医院药剂科;2.济南市第四人民医院放疗科,山东济南,250031) 关键词:阿尔茨海默病;免疫治疗;临床试验;研究进展 中图分类号:R749.16 文献标志码:A 文章编号:1672-2353(2012)13-0144-03 β淀粉样蛋白(Aβ)沉积是老年痴呆最典型的病理特征之一。大量证据表明[1],Aβ沉积和疾病的发生发展具有很强的相关性,AD患者大脑区域的Aβ1-40和Aβ1-42含量几乎与其认知能力损伤具有定量的相关性。Aβ蛋白、Aβ分子寡聚体、Aβ斑块具有很强的神经毒性,可活化神经胶质细胞,诱导神经元的凋亡、神经突触形成不良等改变,最终引起一系列的病理改变[2-3]。因此,“Aβ假说”成为AD发生发展的主要假说。研究者认为,可以通过减少淀粉样蛋白的产生、降低其寡聚物的稳定性、加速斑块的清除等环节进行干预,以减少淀粉样蛋白的毒性,改善AD的病理进程。利用免疫学方法对Aβ及Aβ斑块进行清除是AD药物治疗研究中的一项重大突破,已有来自动物实验的证据表明[4-5],针对Aβ的主动免疫或被动免疫可以清除AD动物大脑组织内过量的Aβ,不少此类药物已经进入临床试验阶段,甚至有的已进入Ⅲ期。本文将对临床试验阶段的AD免疫治疗方面的药物进行综述,期待不久的将来,这类药物可以真正使AD患者受益。 1 AD免疫治疗机制 目前对AD治疗的免疫学方法有主动免疫和被动免疫2种方式,各有其优势及不足。 1.1 主动免疫 用人工合成的Aβ1-42疫苗免疫接种,刺激机体产生抗Aβ1-42抗体,导致单核/小胶质细胞的激活,从而清除Aβ1-42及Aβ斑块,利用这种主动免疫原理设计的Aβ免疫疗法可望成为AD的一种新的治疗方法。1999年Lue等[6]使用Aβ1-42对动物模型实施主动免疫,结果发现不仅Aβ的神经病理学得到了改善,还阻止了认知功能的减退,这为免疫疗法干预脑组织中Aβ含量并引起认知能力改善提供了第一个证据。 2002年抗Aβ疫苗AN-1792临床试验中发现,AN-1792成功使80名健康志愿者及部分家族性AD患者产生免疫应答,然而随后在轻中度AD患者进行的Ⅱ期临床试验由于6%出现了无菌性脑膜脑炎迫中止。这可能是因AN1792疫苗中完整的Aβ1-42同时具有B细胞和T细胞识别的抗原表位,导致自身特异性Th1淋巴细胞也被活化有关,介导了自身免疫引起的。虽然尸检发现其具有强大的降低Aβ的功能,甚至能完全清除病人脑中的Aβ斑块。 在此基础上,人们认识到作为免疫治疗,并不需要完整的Aβ肽段,针对N末端或中央区域的某部分形成的抗体即可形成对Aβ的保护作用;而且只要刺激机体产生体液免疫,无需细胞免疫的激活也可减轻脑组织的Aβ负荷。于是,对疫苗不断进行改良,通过选择Aβ的特异序列、疫苗表位,挑选人源抗原、使用免疫佐剂等方法,出现了避免神经系统炎症反应和毒性的第二代Aβ疫苗。 CAD-106是一种Qβ病毒性疫苗,含有Aβ1 -6片段,动物实验中可诱导Aβ特异性抗体的产生,减少Aβ斑块的聚集,不激活T淋巴细胞也未引起脑膜脑炎。轻中度AD患者中多次注射CAD-106的安全性及耐受性好,未引起脑膜脑炎。Ⅱa期临床试验中,2/3的受试者,经CAD-106治疗后有产生较高滴度的抗Aβ-IgG抗体,但脑脊液Aβ水平和脑容积与安慰剂组并无差异[7]。目前还有一项Ⅱ期临床试验在进行中。 ACC-001和V-950为针对Aβ肽段N-末端某些序列研发的疫苗,包含有B淋巴细胞表位。ACC-01以突变的白喉毒素CRM19为载体,ACC-01和ACC-001(QS-21)均已在AD 患者中进行Ⅱ期临床试验以观察长期疗效,目前还没有结果报道。V-950,以Aβ多肽序列N端 收稿日期:2012-04-19实用临床医药杂志 ·144·Journal of Clinical M edicine in Practice2012年第16卷第13期
发布日期20071130 栏目化药药物评价>>临床安全性和有效性评价 上市前药物临床安全性评价与风险评估(五)--临床试验安全性数据的总结与评标题 价 作者杨焕 部门 正文内容 审评五部杨焕 摘要:风险评估即患者获益与风险比最大化的管理思路应贯穿于药物 的整个生命周期。任何一个新药的风险评估都涉及到数量和质量两个 方面,数量是指安全性数据库的规模;质量是指临床试验设计、实施、 结果分析全过程的质量,在安全性方面具体是指对于药物不良反应报 告、归类、判断、分析总结的质量。本系列文章从技术评价角度,在 分析了解国内外药物不良反应监测的历史与发展的基础上,对上市前 安全性数据库的规模大小和如何保证安全性数据库的质量方面问题进 行了探讨,同时也参考和介绍了国外发达国家最新的风险评估和风险 控制理念,其目的是为临床试验的研究者和注册申请人提供参考和建 议。
关于临床试验中的安全性数据如何进行总结与评价,自上世纪90年代ICH就相继发布了药品注册的国际技术要求,如ICHE2/E3/E6/E9的内容;国内SFDA在2005年也相继发布了《化学药物临床试验报告的结构与内容技术指导原则》和《化学药物和生物制品临床试验的生物统计学技术指导原则》,建议同时参考相关内容。 一、安全性数据的总结和分析 一般原则上要求,只要使用过至少一次受试药物的受试者均应列入安全性分析集。对安全性数据的分析总结应在三个层面加以考虑。首先,必须确定受试者用药/暴露(exposure)的程度,指试验药物的剂量、用药时间,用药的受试者人数,来决定研究可在多大程度上可以评价安全性;其次,确认常见的不良反应、异常改变的实验室检查指标,通过合理的方法进行分类,以合适的统计方法再比较各组间的差异,通过各治疗组之间比较分析出那些可能影响不良反应/不良事件发生频率的因素,如时间依赖性、与剂量或浓度关系、人口学特征等;最后,通过分析因不良事件(不管是否与药物有关)而退出研究或已死亡的受试者进行分析,来确定严重不良事件和其他重度不良事件(指需要采取临床处理,如停药、减少剂量和其他治疗手段的不良事件)。 所有不良事件应明确与药物的因果关系。建议以图表的方式对出现的不良事件进行总结;对患者个体数据列表;对重点关注的不良事件进行详细地描述。受试药和对照药出现的不良事件均应报告。 1. 用药/暴露的程度
广东省药学会药物临床试验专业委员会 安全评价?广东共识(2016) (广东省药学会2016年7月25日印发) 起草说明 药物临床试验的安全性评价是全面、客观评价一个试验药物不可或缺的内容。安全信息的收集、评价和记录主要由研究者团队完成,但申办者所撰写的研究方案和制定的实施细则是确保高质量信息收集和整理等工作的关键性因素。 药物临床试验过程中,安全性评价环节一直是研究各方存在争议的部分。但迄今,在信息发现、收集和评价过程中尚缺乏共识、指南或标准供研究者借鉴与遵循,因此,在研究方案具体实施过程中,各申办方常采用各自不同的操作方法和评价标准。为了明确临床试验过程中药物安全性评价相关概念、原则和方法,增加研究的可操作性,以期提高药物临床试验安全信息质量并规范评价方法,本专委会特组织专家、同道共同讨论、撰写,形成此共识以供借鉴。作为一次初步尝试,本共识仍存在不足之处,望与业内专家及同道一起,结合具体实践不断修订与完善。 本共识撰写工作由曹烨、万邦喜共同发起、组织和撰写。来自跨国制药企业的7位同行(李艳等)和医疗机构的3位研究者(中山大学附属肿瘤医院徐立医生、陈功医生、张阳医生)参与审阅。在专委会广泛征求意见期间,得到专委会主任委员洪明晃教授的悉心指导,收到“肿瘤医院联盟”、“药物警戒在中国群”以及很多专家同行的建设性修改意见。在此向各位专家的无私付出表示衷心感谢! 共识撰写小组 2016年6月30日
目录 一、总则 (4) 二、定义 (4) 1.不良事件的定义与类别[1][2][3] (4) 2.严重不良事件[3][4][5] (5) 3.重度不良事件与严重不良事件[1][3][4] (6) 4.可疑的、非预期的严重不良反应[4][6][7] (6) 三、不良事件/严重不良事件的收集、记录、描述 (7) 1.不良事件名称的确定[2][8][9] (7) 2.不良事件的开始时间[2][4][6][8] (7) 3.不良事件的随访[10][11] (8) 4.不良事件的结束时间[2][6] (8) 5.不良事件的转归[2][12] (8) 6.不良事件的合并用药[8][13] (9) 7.不良事件/严重不良事件的记录与描述[2][14][15] (9) 8.反复发生的不良事件[2][16] (9) 9.不良事件的严重程度[3][17] (10) 四、不良事件/严重不良事件的相关性判断[2][3][11][18][19] (10) 五、严重不良事件处理原则与报告时限[18] (11)
NSCL-C#1 - 放射治疗原则 I.一般原则 (见表1.放射治疗常用缩写) ?应该由通过职业认证、临床实践中主要从事肺癌放疗的放射肿瘤学家确定合理的放疗(RT)。 ?作为根治性或姑息性治疗,在所有分期的非小细胞肺癌中放疗均有潜在的作用。作为多学科评估或讨论的一部分,对于所有III期NSCLC、因内科因素不能手术的早期疾病、拒绝手术或高危手术候选者,以及可能受益于局部治疗的IV期疾病患者,均应让放射肿瘤学参与。 ?现代放疗的关键目的是肿瘤控制最大化,同时使治疗毒性最小化。最低技术标准是根据CT设计的三维适形放疗。 ?当需要安全的根治性放疗时,可合理使用更先进的技术。这些技术包括(但不限于)4D-CT和/或PET/CT模拟、IMRT(调强放疗)/VMAT(旋转容积调强放疗)、IGRT(影像引导放射治疗技术)、运动管理及质子治。采用先进技术与老旧技术 的非随机对照证明,降低毒性并改善生存。在一项根治性化/放疗治疗III期NSCLC的前瞻性试验(RTOG 0617)中,与三维适形放疗相比,尽管调强放疗组IIIB期比例较高且治疗体积较大,但是,调强放疗降低高级别放射性肺炎近 60%(从7.9%降低到3.5%)而生存和肿瘤控制结果相似;因此,在这种情况下,适 形调强放疗优于三维适形放疗。 ?使用先进技术的中心应实施并记录具体的质量保证措施。治疗计划与交付两者均外部认证是理想的,就像RTOG临床试验采用先进技术所要求的那样。 II.放射治疗模拟、计划和交付 ?应使用适当固定设备在放疗位置获得的CT扫描进行模拟,在中心型肿瘤或淋 巴结病变的患者中,为更好地勾画靶/器官,推荐静脉造影±口服对比剂。由于静脉造影可以影响组织的非均匀性校正计算,因此,当进行强烈增强时,可能需要密度蒙罩或使用增强前扫描。 ? PET/CT明显提高靶标精度[6],尤其是对于显著肺不张和有静脉造影CT禁忌 症的患者。一项对比PET/CT与单纯CT制定放疗计划的随机试验证明,PET/CT 放疗计划可增加排除徒劳无效的根治性放疗、减少复发并且有改善总生存的趋势。考虑到NSCLC的快速发展潜力,应最好在治疗前4周内获得PET/CT。理想情况下,获得治疗位置的PET/CT。
464中国临床药理学杂志 第25卷第5期2009年9月(总第12l期) 新药上市前临床试验安全性数据的分析与评价 Clinicalsafetydataanalysisandevaluationofnewdurgsinthepre-approvalphase 杨焕 (国家食品药品监督管理局药品审评中心,北京100038) YANGHuan (CenterforDrugEvaluation,StateFoodandDrugAdministration.Beijing100038,China) 收稿日期:2009—02—17 修回日期:2009—07—14 作者简介:杨焕(1970一),女,副主任医师,主要从事药品技术审评工作 通讯作者:杨焕 Tel:(olo)68585566 E—mail:yanshuman@cde.orgycn摘要:本文分析了上市前药物临床试验进行不良反应监测与评价的特点,介绍了安全性数据的分析、总结和评价方法,阐明了临床试验中需要特别关注和要评价的安全性问题,强调风险评估(即患者获益与风险比最大化)的管理思路应贯穿于药物的整个生命周期中。 关键词:新药;上市前临床试验;安全性数据 中图分类号:R954文献标识码:C 文章编号:1001—6821(2009)05—0464—03 关于临床试验中的安全性数据如何进行总结、分析与评价,自20世纪90年代以来,人用药品注册技术要求国际协调会(ICH)就相继发布了药品注册的国际技术要求,如ICH中的E2/E3/E6/E9,均涉及此方面的内容¨o;国家食品药品监督管理局(SFDA)在2005年也相继发布了《化学药物临床试验报告的结构与内容技术指导原则》和《化学药物和生物制品临床试验的生物统计学技术指导原则》心-3],建议同时参考。 1上市前临床药物不良反应监测与评价的特点 上市前的临床试验是对药物的有效性、安全性进行科学的评价,是新药开发的重要环节,为国家药品监督管理部门批准其生产上市提供依据。《药品I晦床试验管理规范》(GCP)是指导和规范药物临床试验过程的法规性文件MJ,可以有效地保证临床试验结果的科学可靠,保护受试者的权益和安全。上市前药物临床试验中的安全性评价作为关键环节,同样必须遵循GCP的要求。 1.1GCP中的有关安全性评价的要求 GCP中的临床试验方案、研究者职责、申办者(注册申请人)职责、监查员的职责、记录与报告等章节,都包含对安全性数据收集和管理(即药物不良反应监测)的具体要求,由此可见对药物安全性评价的要求,贯穿整个GCP的实施中。 1.2药物上市前不良反应监测的特点 药物不良反应监测的特点有以下5种:①在新药临床试验期问,因用药单一并用于特定目标人群和针对惟一的适应证,对于出现的不良事件较好归因。②药物不良反应定义有所不同,上市前临床研究中,由于正在进行研究的试验药物的用药剂量、疗效等均未完全确定,因此,任何剂量下出现的与药物有关的、有害的且非期望的反应,都应当视为药物不良反应,这与世界卫生组织(WHO)对于上市后药物不良反应的定义有一定的差异。③上市前临床试验中的不良反应/不良事件(ADR/AE)报告,均来自有目的、明确的前瞻性临床研究,这使得ADR/AE关联性评价较上市后易于判断。④上市前临床试验中,更强调对个例严重且非预期不良反应的快速报告和评价。 万方数据
药物临床试验期间安全性数据快速报告 常见问答 版本号: 1.0 ) 药品审评中心 2019 年4 月
2018 年1月25 日原国家食品药品监督管理总局发布了《关于适用国际人用药品注册技术协调会二级指导原则的公告》,要求“自2018 年5 月1 日起,药物临床研究期间报告严重且非预期的药品不良反应适用《E2A: 临床安全数据的管理:快速报告的定义和标准》《:监管活动医学词典()》和《E2B ( R3 ): 临床安全数据的管理:个例安全报告传输的数据元素》。” 2018 年4 月27 日药品审评中心发布了《药物临床试验期间安全性数据快速报告的标准和程序》,进一步明确了我国药物临床试验期间非预期严重不良反应 ()快速报告的重点内容和报告途径。 本问答文件是在上述基础上,对于我国药物临床试验期间安全性数据快速报告实施以来部分共性问题的统一解释和澄清,供申请人/ 参考和遵循。 随着快速报告工作的逐步完善,本问答文件后续也将不 断进行增补和更新,在使用过程中,需注意采用最新的版本
目录 █快速报告的范围?????????????????????????? 3 █快速报告的时限????????????????????????? 6 █ 提交方 式???????????????????????????? ? 7 █ 关于购买第三方服务???????????????????????8 █ 账户申请及测试????????????????????8 █ 申请人之窗与格式文 件??????????????????9 █ E2B 数据元素相关要 求????????????????????? 11 █ 破盲与阳性对照药、安慰剂报告问题????????????? 11 █ 受理号填 写???????????????????????????? 13
肿瘤免疫治疗在研药物靶点概览 Overview of innate and adaptive checkpoint pathways 免疫治疗是指通过免疫系统达到对抗癌症目的的治疗方式,也是生物治疗的一种。识别和杀死异常细胞是免疫系统的天然属性,但是癌症细胞经常有逃避免疫系统的能力。过去几年,癌症免疫领域的快速发展产生了几种治疗癌症的新方法,通过增强免疫系统中某些成分的活性或者解除癌症细胞对 免疫系统的抑制来发挥作用。广义的免疫治疗包括免疫检查点抑制剂、免疫细胞治疗、溶瘤病毒、治疗性抗体、癌症疫苗以及免疫系统调节剂。肿瘤免疫治疗近来备受关注,除了手术、化疗及放疗外,已成为癌症治疗的重要手段。Ipilimumab及nivolumab / pembrolizumab是最早上市的免疫检查点抑制剂类药物,分别靶向于CTLA-4及PD-1;在 治疗非小细胞肺癌及黑色素瘤领域已逐渐从二线转变为一 线治疗药物。免疫治疗药物并非没有弱点,药物的试用可能会诱导肿瘤细胞额外免疫检查点活性的上调,凸显了开发新型抗肿瘤免疫激活剂的重要性。新出现的药物不仅通过封闭免疫抑制性检查点或作为免疫刺激信号通路的激活剂而靶 向于获得性免疫淋巴细胞,还可靶向于先天免疫过程中的巨噬细胞和自然杀伤细胞,两者广泛存在于多种类型的实体瘤及血液系统癌症中。本文将对新出现的进入临床研究或临床
前研究的肿瘤免疫治疗靶点做一概览。 表1. Summary of past and current clinical trials in cancer for immune checkpoint agents(本表来源于文献1,篇幅所限,对更多信息感兴趣的读者可查阅原文)获得性免疫-抑制性淋巴细胞受体Ligand interaction and structural similarities between LAG3 and CD4 LAG-3LAG-3 (lymphocyte activation gene 3,LAG-3, CD223)和CD4是同源蛋白,但是以更高的亲和力与主要组织相容性复合体Ⅱ类分子(major histocompatibility complex classⅡ,MHCⅡ)结合,主要表达在活化的T淋巴细胞、B淋巴细胞、自然杀伤细胞(natural killer cell,NK)和浆细胞样树突状细胞(plasma cytoid dendriticcells,pDCs),并负调控T 细胞功能。研究表明LAG-3选择性地上调Treg表面的CD4,因此LAG-3抗体在体内可降低Treg活性。抑制或敲除 LAG-3会解除Treg对T细胞的抑制功能。另外,在缺少CD4+T细胞的情况下,LAG-3抗体能够增加CD8+T细胞的功能。T细胞失能或者耗竭时会表达多种免疫检查点分子,在慢性感染模型及自身抗原识别模型中LAG-3和PD-1通常都有共表达现象。协调抑制LAG-3及PD-1能够增强免疫应答,因此目前关于LAG-3抗体的临床试验都是单独或者与PD-1联用来观察效果。目前主要有以下几家公司进行LAG-3的临床试验:BMS的BMS986016,Regeneron和Sanofi
肿瘤放射治疗学期末考 试重点笔记 文件管理序列号:[K8UY-K9IO69-O6M243-OL889-F88688]
恶性肿瘤的临床治愈率为45℅,其中外科占22℅,放射治疗占18℅,化学治疗占5℅ 根据肿瘤的放射敏感性分类: 1、放射高度敏感的肿瘤:恶性淋巴瘤、睾丸精原细胞瘤、肾母细胞瘤、尤 文肉瘤、小细胞肺癌 2、放射中度敏感的肿瘤:鳞状细胞癌、宫颈癌、宫体癌、乳腺癌、皮肤 癌、肾移行细胞癌 3、放射低度敏感的肿瘤:胃肠道的腺癌、胰腺癌、前列腺癌 4、放射敏感性较差的肿瘤:纤维肉瘤、脂肪肉瘤、横纹肌肉瘤、恶性纤 维组织细胞瘤 放射治疗的禁忌症 1、全身情况 (1)心、肝、肾等重要脏器功能严重损害时; (2)严重的全身感染、败血症或脓毒血症未控制者; (3)治疗前血红蛋白<80g/L或白细胞<3.0×109/L未得到纠正者;(4)癌症晚期合并贫血、消瘦或处于恶病质状态,评估生存期不足3至6月者。 2、肿瘤情况 (1)肿瘤情况已出现广泛转移,而且该肿瘤对射线敏感性差,放射治疗不能改善症状者;(2)肿瘤所在脏器有穿孔可能或已穿孔时;(3)凡属于放射不敏感的肿瘤应视为相对禁忌症。 3、放射治疗情况
(1)近期曾做过放射治疗;(2)皮肤或局部组织纤维化;(3)皮肤溃疡经病理证实阴性;(4)不允许再行放射治疗者。 根治性放射治疗:是指通过给予肿瘤致死剂量的照射,使肿瘤在治疗区域内缩小、消失,达到临床治愈的效果。 接受根治性放射治疗的患者要符合以下条件:1、一般状况好2、局部肿瘤较大并无远处转移;3、病理类型属于对射线敏感或中度敏感的肿瘤。术前放射治疗的目的是:1.通过一定剂量照射使肿瘤细胞的活性降低,防止手术中引起肿瘤细胞的种植转移和播散;2.使肿瘤缩小、降低临床分期,便于手术切除;3.控制肿瘤周围的亚临床病灶和区域的淋巴结,提高手术的切除率;4.使原本不能切除的病灶通过放射治疗也能够进行根治性切除。 在放射治疗结束后10天或放射治疗后2-4周手术,可以使组织有充分的修复时间,此时急性放射反应已经消失,慢性放射反应还未发生,这期间既不会给手术造成困难,也不会影响术后切口愈合。 术后放射治疗,一般在手术后2至4周内尽早开始。 远距离放射治疗:亦称外照射,是指放射源发出的射线通过体外某一固定距离的空间,并经过人体正常组织及邻近器官照射到人体某一病变部位的放射治疗方式。可分为等中心放射治疗技术(源轴距照射技术,SAD)和源皮距治疗技术(SSD) 三维适形放射治疗(3D-CRT)是一种高精度的放射治疗技术,具有以下优势:
临床试验 代表含义:指任何在人体(病人或健康志愿者)进行药物的系统性研究,以证实或揭示试验药物的作用、不良反应及/或试验药物的吸收、分布、代谢和排泄,目的是确定试验药物的疗效与安全性。 Ⅰ临床研究 代表含义:首次在人体进行研究药物的周密试验计划,受试对象是少量(开放20~30例)正常成年健康自愿者。目的是观察药物在人体内的作用机制。 Ⅱ临床研究 代表含义:在只患有确立的适应症的病患者(盲法不小于100对)上进行的研究,目的是找出最佳的剂量范围和考虑治疗可行性 Ⅲ临床研究 代表含义:确定研究药物的有效性和安全性、受益和危害比率。(试验组不小于300例。) Ⅳ临床研究 代表含义:新药获准注册上市后的大型研究,检察普遍临床使用时的不良反应和毒性。 药品临床试验管理规范 代表含义:对临床试验的设计、实施和执行,监查、稽查、记录、分析和报告的标准。该标准是数据和报告结果的可信和精确的保证;也是受试者权益、公正和隐私受保护的保证。 伦理委员会 代表含义:是指一个由医学,科学专业人员及非医学,非科学人员共同组成的独立体,其职责是通过对试验方案、研究者资格、设备、以及获得并签署受试者知情同意书的方法和资料进行审阅、批准或提出建议来确认临床 试验所涉及的人类受试者的权益、安全性和健康受到保护,并对此保护提供公众保证。 申办者 代表含义:发起一项临床试验,并对该试验的启动、管理、财务和监查负责的公司、机构或组织。 研究者 代表含义:实施临床试验并对临床试验的质量及受试者安全和权益的负责者。研究者必须经过资格审查,具有临床试验的专业特长、资格和能力。 协调研究者 代表含义:在多中心临床试验中负责协调参加各中心研究者工作的一名研究者。 监查员 代表含义:由申办者任命并对申办者负责的具备相关知识的人员,其任务是监查和报告试验的进行情况和核实数据。合同研究组织 代表含义:一种学术性或商业性的科学机构。申办者可委托其执行临床试验中的某些工作和任务,此种委托必须作出书面规定。
细胞因子在免疫治疗中的应用概述 细胞因子一般是由受到刺激的细胞产生,主要为免疫细胞。细胞因子具有高效性,在微摩尔甚至皮摩尔都可以起作用。单个细胞因子对免疫的作用取决于如下的条件:局部细胞因子浓度、其受体表达的模式及多个信号通路在免疫应答细胞中的整合。细胞因子作为分子信使,允许免疫系统细胞彼此通信,以产生对靶抗原的协调,在许多疾病中具有调节和效应功能,因此细胞因子及其受体可用于免疫治疗。 在免疫治疗过程中,细胞因子直接刺激肿瘤部位的免疫效应细胞和基质细胞,增强细胞毒性。通过对动物肿瘤模型研究,发现细胞因子具有广泛的抗肿瘤活性,已经有很多细胞因子用于癌症的治疗。获得FDA批准上市的细胞因子药物已有多个,如高剂量的IL-2用于治疗黑素瘤和肾细胞癌,IFN-α用于III期黑素瘤的辅助治疗。还有更多的细胞因子已经进入临床试验阶段,如GM-CSF、IL-7、IL-12、IL-15、IL-18和IL-2。 细胞因子作为一种免疫调节剂,可以用于激活免疫疗法、抑制免疫疗法等,包括各种重组、合成和天然的制剂。如白细胞介素类(IL-2、IL-7、IL-12),趋化因子(CCL3、CCL26、CXCL7)及其它细胞因子(干扰素、粒细胞集落刺激因子)等。 在激活免疫疗法中 如粒细胞集落刺激因子(G-CSF)可以刺激外周血干细胞(从病人血液中提取)产生淋巴细胞,经过体外与肿瘤抗原共培养后,再输回到病人体内,并结合刺激性的细胞因子以增强免疫效应,这样的细胞就可以摧毁携带相同抗原的肿瘤细胞,从而达到治疗的效果。 白细胞介素-2可以与抗CD3和同种异体反应性细胞融合,生成过继T细胞。这种细胞可以转移到患者体内,可以进一步提高IL-2的抗癌活性。白细胞介素-7和白细胞介素-2可以用来恢复免疫功能缺陷患者的免疫系统,这一研究已经进如临床试验阶段。 在抑制免疫疗法中
放射治疗与辐射损伤 放射治疗(放疗)是恶性肿瘤的主要治疗手段之一。但放射线是一把双刃剑.它既能杀灭肿瘤细胞. 同时又不可避免地造或正常组织的损伤。因此在肿瘤的放疗中。认识和掌握放射线对正常组织的 损伤作用是非常重要的: 从理论上讲,只要给予足够的剂量,放疗是能够完全控制肿瘤的:但在临床实际中,肿瘤周 围的正常组织对放射线的耐受能力限制了照射剂量。也就是说,我们在肿瘤放疗中给予的照射 剂量往往是肿瘤周围的正常组织所能够耐受的最大剂量。而不是完全杀灭肿瘤所需的剂量,即在控制肿瘤(治疗益处)和正常组织损伤(危害)之间寻找平衡点。忽视了任何一方,不但可能达不到放疗所应达到的治疗效果,反而可能因治疗的不良反应给患者带来损害。为了在尽量提高放疗疗效的同时,使肿瘤周围的正常组织少受损伤,当前临床上普遍采取以下手段: 1.利用先进的放疗设备和新的治疗手段实施精确放疗,包括精确定位、精确计划、精确投照主要方法有三维适形放疗(3D—CRT),调强放疗(LMRT),影像引导放疗(IGRT)。螺旋断层放疗。立体定向放射外科(X刀、γ刀)等。 2.使用放射增敏剂,提高肿瘤细胞对放射线的敏感性,提高疗效。 3.使用放射保护剂: 降低正常组织对射线的敏感性,提高正常组织对放射剂量的耐受性,如部分外用护肤品。使用治疗辐射损饬的药物(如目前国家唯一正式批准可用于辐射损伤的安多霖胶囊),促进正常组织的修复,提高放疗疗效,减轻近期放射损伤的程度.降低晚期放射损伤的发生率。4.改变常规放疗分割方式:如采用超分割放疗以降低晚期放疗反应的发生率总之,在放疗期间,采用先进的仪器设备并配合服用可以用于辐射损伤的药物,对增加疗效,降低不良反应,保证放疗的正常进行,减少肿瘤的复发和转移,都有着很重要的,作用和意义。 放疗与手术或化疗间想和配合治疗 恶性肿瘤常规治疗手段有手术、放料及化疗。与其他治疗手段一样,肿瘤放疗有其优点也有其局限性,由于恶性肿瘤的生物学特性及目前尚缺乏有效的特异性手段来早期发现肿瘤。因此目前肿瘤的治疗需要多种手段相结合。 放疗联合外科手术的综合治疗模式 放疗作为局部无创性治疗手段,对患者的一般情况要求不高,即使患者合并有交严重的其他脏器疾病或肿瘤侵犯到大血管和重要脏器,手术可能成为禁忌,多数仍可以耐受治疗。另外,放疗对正常组织的保护较手术为好。两者综合治疗的模式有: ⑴术前放疗:其优点是放疗可使肿瘤缩小,减少手术野内肿瘤细胞的污染,缩小手术切除 范围,降低肿瘤细胞的活力,减少手术所致的医源性播散。 ⑵术中放疗:术中切除大块肿瘤后,在直视下对瘤床及(或)周边的淋巴引流区域进行一次大剂量照射,可使照射野外的正常组织得到很好的保护,同时给与肿瘤靶区较高照射剂量。多数情况下仍需加用术后外照射放射。 ⑶术后放疗:可消灭手术野内外的残留病灶及亚临床病灶,可根据术后肿瘤的病理学诊断,设计合理的放疗方案。 ⑷术前放疗联合术中及术后放疗。