375
? Springer Science+Business Media New York 2016
L. Ganti (ed.), Atlas of Emergency Medicine Procedures , DOI 10.1007/978-1-4939-2507-0_65
P ostextraction Hemorrhage M ichael A .A braham ,A mir A zari ,J ennifer W estcott ,and F ranci S tavropoulos 65.1I ndications ? R ecent tooth extraction site, presenting with more than a slight oozing of blood ? F ull evaluation indicating amount of blood loss, present physical condition, and reason for hemorrhage including coagulopathy or medication use 65.2C ontraindications ? A bsolute –N one ? R elative –N one 65.3M aterials and Medications ? 2× 2 gauze pad ? S aline ? 25-gauge needle, syringe ? L ocal anesthetic without vasoconstrictor—2 % lidocaine plain ? G elfoam ? (absorbable gelatin-compressed sponge) or
oxidized cellulose
? T opical thrombin ? S uture kit with 3-0 chromic gut suture or 3-0 Vicryl ?
suture (synthetic absorbable sterile surgical suture com-posed of a copolymer made from 90 % glycolide and 10 % l -lactide) ? H emostat 65.4P rocedure 1. U se suction and saline irrigation to gently rinse the
affected area. If a “liver” clot is present, irrigate and remove it with suction. 2. D etermine the source of hemorrhage without local anes-thesia, if possible, because the use of local anesthetic
with an added vasoconstrictor may obscure bleeding
sites. 3. M oisten a folded 2 × 2 gauze pad with saline and place it directly onto the extraction site. 4. I nstruct the patient to apply ? rm biting pressure, and observe for 1 h, changing gauze as necessary. 5. I f bleeding persists, an intraoral nerve block should be
performed.? B locks are preferred to in? ltrations; anesthetic with epinephrine in? ltrated near the bleeding site will pro-duce only temporary local hemostasis from vasoconstriction. 6. G ently curette the tooth extraction socket and remove areas of old blood clot or granulation tissue. 7. C heck soft tissue for associated arterial bleeding.? I f hemorrhage is localized to soft tissue, use pressure
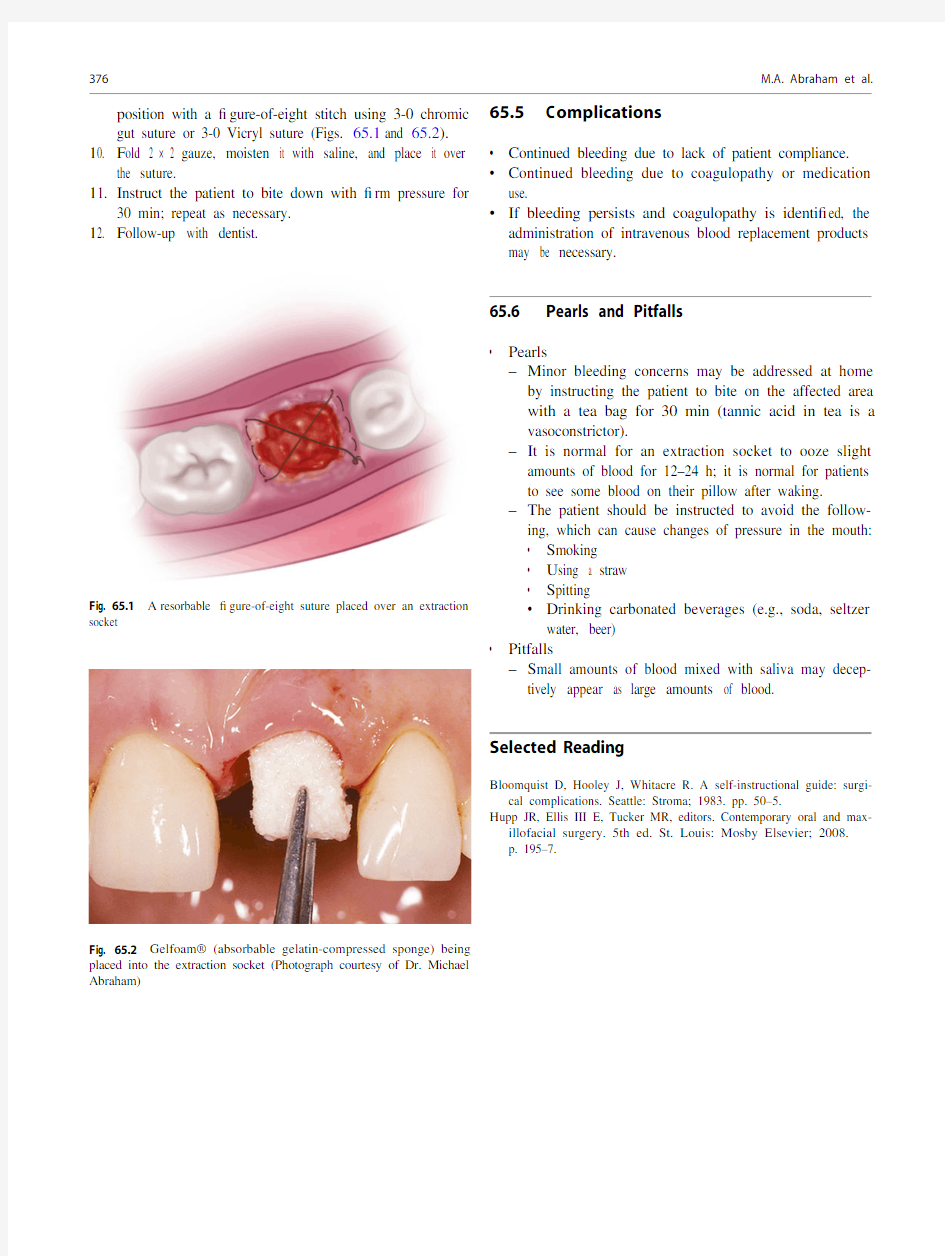
or tie off vessels. 8. F old Gelfoam ? into a small cylinder to ? t into the extrac-tion socket. 9. P lace Gelfoam ? with topical thrombin or Surgicel ?
(absorbable hemostat) into the socket and hold in M . A . A braham ,D MD (*)
U nited States Air Force, Dental Corps ,M inot ,N D ,U SA e -mail: mikeabrahamdmd@https://www.doczj.com/doc/b417794319.html, A . A zari ,D MD D epartment of Oral and Maxillofacial Surgery , O regon Health and Science University ,P ortland ,O R ,U SA e -mail: Azari@https://www.doczj.com/doc/b417794319.html,
J . W estcott ,D MD P rivate Practice ,P alm Beach Gardens ,F L ,U SA e -mail: Jwestcott561@https://www.doczj.com/doc/b417794319.html,
F . S tavropoulos ,D DS
D epartment of Dental Specialties – Oral and Maxillofacial Surgery, Gundersen Health System ,L a Crosse ,W I ,U SA
e -mail: Mfstavro@https://www.doczj.com/doc/b417794319.html,
65
376
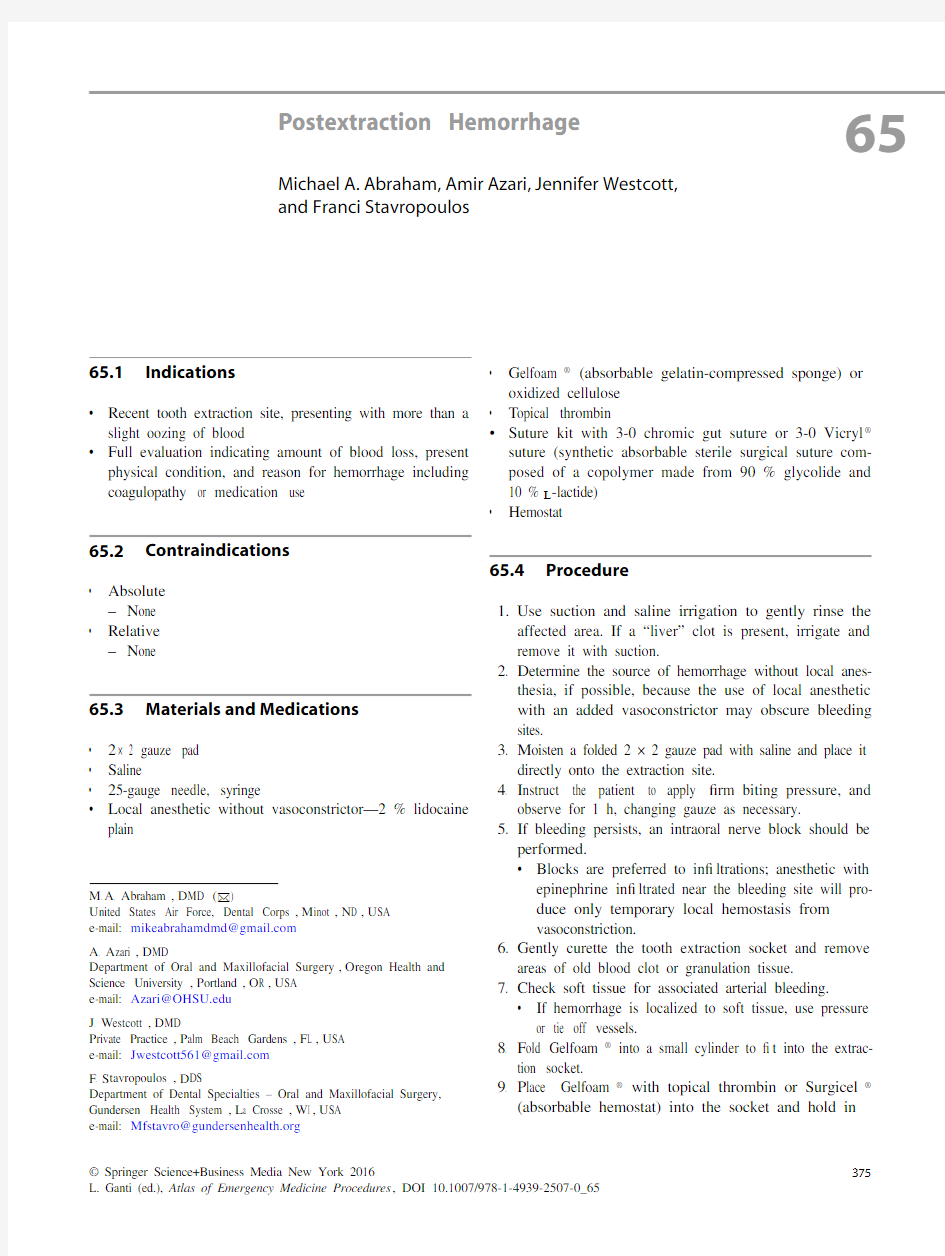
p osition with a ? gure-of-eight stitch using 3-0 chromic gut suture or 3-0 Vicryl suture (Figs. 65.1and 65.2). 10. F old 2 × 2 gauze, moisten it with saline, and place it over
the suture.
11. I nstruct the patient to bite down with ? rm pressure for
30 min; repeat as necessary.
12. F ollow-up with dentist. 65.5C omplications
? C ontinued bleeding due to lack of patient compliance. ? C ontinued bleeding due to coagulopathy or medication use.
? I f bleeding persists and coagulopathy is identi? ed, the administration of intravenous blood replacement products may be necessary.
65.6 P earls and Pitfalls
? P earls
–M inor bleeding concerns may be addressed at home by instructing the patient to bite on the affected area
with a tea bag for 30 min (tannic acid in tea is a
vasoconstrictor).
–I t is normal for an extraction socket to ooze slight amounts of blood for 12–24 h; it is normal for patients
to see some blood on their pillow after waking.
–T he patient should be instructed to avoid the follow-ing, which can cause changes of pressure in the mouth:
? S moking
? U sing a straw
? S pitting
? D rinking carbonated beverages (e.g., soda, seltzer water, beer)
? P itfalls
–S mall amounts of blood mixed with saliva may decep-tively appear as large amounts of blood.
S elected Reading
B loomquist D, Hooley J, Whitacre R. A self-instructional guide: surgi-
cal complications. Seattle: Stroma; 1983. pp. 50–5.
H upp JR, Ellis III E, Tucker MR, editors. Contemporary oral and max-
illofacial surgery. 5th ed. St. Louis: Mosby Elsevier; 2008.
p. 195–7.
F ig. 65.1 A resorbable ? gure-of-eight suture placed over an extraction
socket
F ig. 65.2
G elfoam? (absorbable gelatin-compressed sponge) being
placed into the extraction socket (Photograph courtesy of Dr. Michael
Abraham)
M.A. Abraham et al.